
SLIDE 1
10/27/2016 1
NON-INVASIVE PRENATAL SCREENING
Mary E. Norton MD Professor of Obstetrics, Gynecology, and Reproductive Sciences University of California, San Francisco October 27, 2016
Disclosure
- Research support from Natera
- No other conflicts of interest
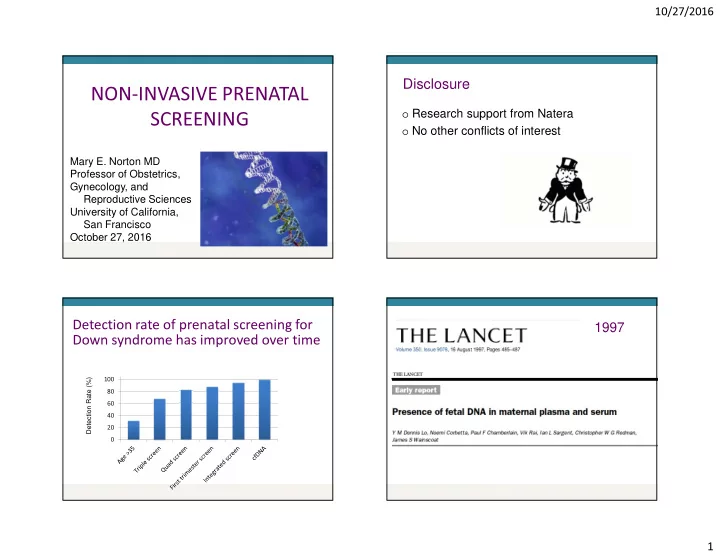
20 40 60 80 100 120
Detection rate of prenatal screening for Down syndrome has improved over time
Detection Rate (%)