
SLIDE 1
1 Robert P Hasserjian, MD Associate Professor Massachusetts General Hospital and Harvard Medical School
Advances in the Diagnosis of Myeloproliferative Neoplasms Discolosures
- Consulting income from Promedior, Inc.
Myeloproliferative neoplasms
- Clonal hematopoietic stem cell disorders
- “Overexuberant” production of one or more
hematopoietic cell types
- Erythroid and granulocytic elements generally
appear normal, without dysplasia
- Treated differently from other myeloid
neoplasms
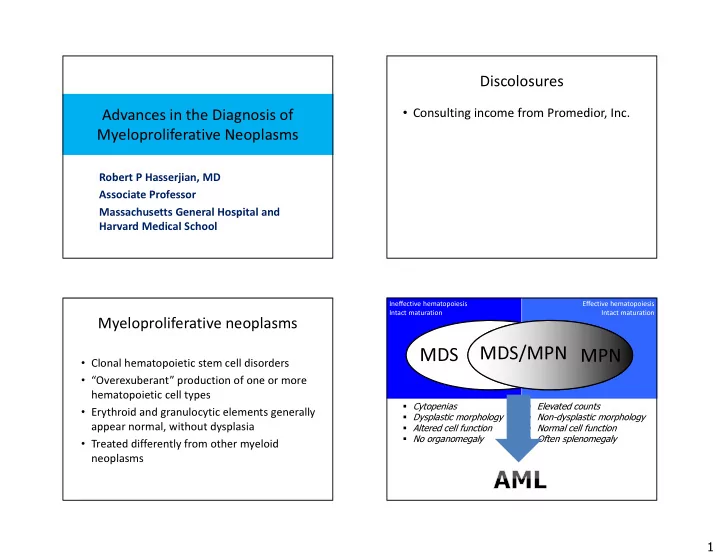
Ineffective hematopoiesis Intact maturation
MDS
Cytopenias Dysplastic morphology Altered cell function No organomegaly
Effective hematopoiesis Intact maturation
MDS/MPN MPN
Elevated counts Non-dysplastic morphology Normal cell function Often splenomegaly