SLIDE 10 Sean N. Parker Center for Allergy & Asthma Research
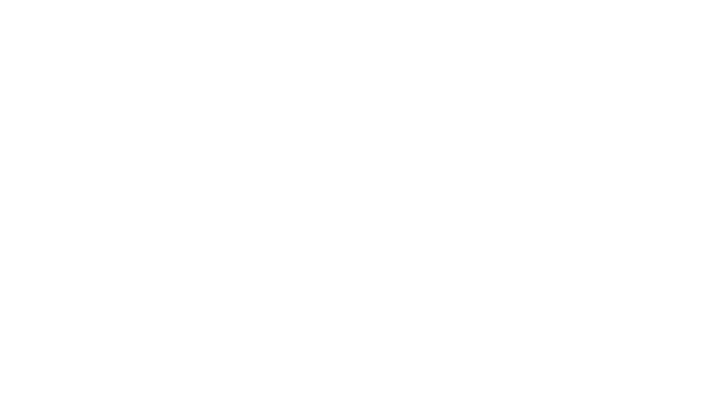
Immune tolerance to oral antigens in the gut
Yu, et al, Nature Rev Immun 2016
M cell IL-10 production Treg cell proliferation Gut homing DC migration Antigen sampling High microbial diversity TGFβ and retinoic acid production α4β7 IL-10, TGFβ IL-10, TGFβ IgA CTLA4 Naive CD4+ T cell CD103+ DC CD103+ Tu cell Lumen Food allergen MHC Peptide Mast cell Dimeric IgA CX3CR1+ macrophage Draining lymph node Gut lamina propria Peyer’s patch Treg cell Treg cell B cell Intestinal epithelial cell Transcytosis
Anergy Apoptosis TH2 cell TFH cell B cell Antigen transfer Filamentous bacteria
) and retinoic acid, thereby inducing naive T cells to differentiate into . B cell clones expressing antibody specific for food allergen may undergo isotype switching in the secondary lymphoid organs with the aid of follicular T helper By contrast, food allergen-specific IgE
- ral antigens has been reported to lead to the anergy or deletion of antigen-specific T cells, possibly after DC interaction
cells secreting different cytokine combinations favour B cell switch recombination to produce particular antibody isotypes, . The roles of tissue-resident T cells, CD8 T cells and T cells remain to be determined. The relationship between T and conversion between the two has been reported