
SLIDE 1
Indigenous Population in the Americas Mexico 15.7 millions 15% - - PDF document
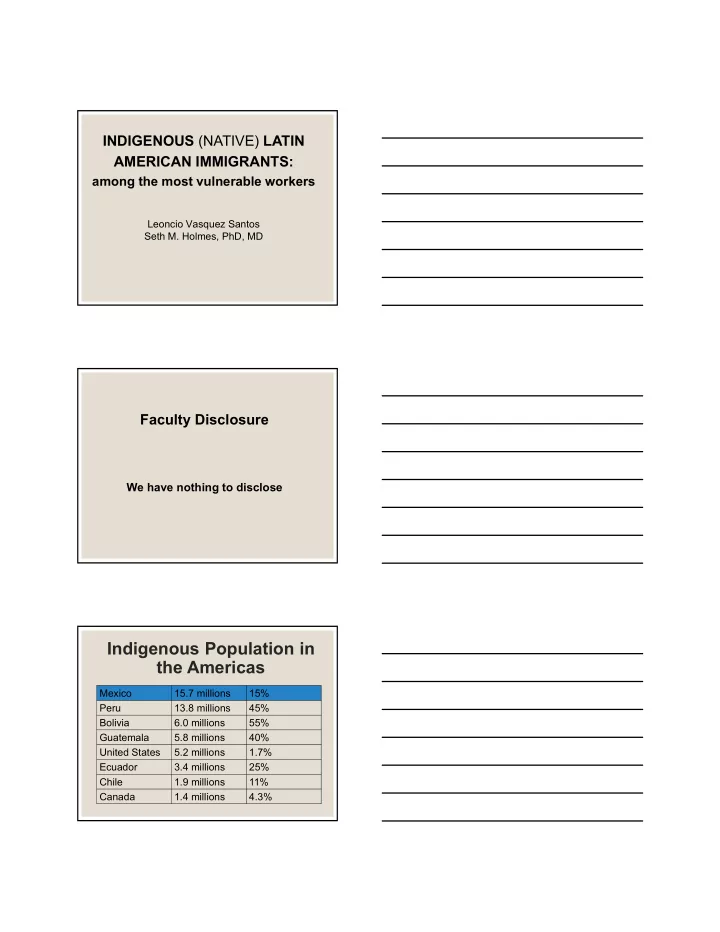
INDIGENOUS (NATIVE) LATIN AMERICAN IMMIGRANTS: among the most vulnerable workers Leoncio Vasquez Santos Seth M. Holmes, PhD, MD Faculty Disclosure We have nothing to disclose Indigenous Population in the Americas Mexico 15.7 millions 15%
are part of the Mesoamerican Pre- Hispanic Cultures.
lineages
math, cosmology
discrimination even in Mexico.
1,000 years of history
remained
Approaches:
medicinal plants/herbs.
pregnancy.
bone problems
muscle pain / sprains
realm of supra-natural conditions
Mexico: (Always)
United States: (’80s)
Program
and found that 50,000 indigenous migrants worked in the fields of California.
number of indigenous persons working in the agriculture sector in California is 120,000 and it reaches 165,000 when children are
demanded and less rewarded jobs (farm work and construction)
long working hours, no toilets with water to wash hands and drinking water.
too often below the minimum wage
Mixtec workers were more likely to accept jobs paying less than the minimum wage and were more likely to be victims of non-payment and other law violations.
bedroom apartments with two or three families (15 people).
around the rivers, mountains and under the
(political, social, economic and religious).
membership and belonging.
“A shift in medical education … toward attention to forces that influence health outcomes at levels above individual interactions.” –Metzl and Hansen 2014 The capacity for health professionals to recognize and respond to health and illness as the downstream effects of broad social, political, and economic structures.
Develop trainees’ capacity in:
health
encounter
clinic
social arrangements that put individuals and populations in harm’s way... The arrangements are structural because they are embedded in the political and economic organization of our social world; they are violent because they cause injury to people.” – Farmer et al. 2006
Metzl and Roberts,
“We argue that, if stigmas are not primarily produced in individual encounters but are enacted there due to structural causes, it then follows that clinical training must shift its gaze from an exclusive focus on the individual encounter to include the organization of institutions and policies, as well as of neighborhoods and cities, if clinicians are to impact stigma-related health inequalities.”
Be g ins Drinking Mo re He a vily Ca n’ t Pa y Re nt, Mo ve s to Stre e t I njury, Ca n’ t Wo rk Be g ins Wo rking a s Da y L a b o re r Mo ve s to Sa n F ra nc isc o I nflux o f Che a p US Co rn; Ca n’ t Ma ke a L iving 4th Ge ne ra tio n Co rn F a rme r in Oa xa c a I n E me rg e nc y De pa rtme nt Afte r F
Ge ts Assa ulte d Standar d Me dic al History & De fault Provide r Inte rpre tation
Nor th Ame r ic an F r e e T rade Agre e me nt (NAF T A) Punitive US immigration Polic y/ Disc rimination City polic ie s c ontributing to high re nts & displac e me nt No He alth Insuranc e (e xc lude d fr
Be g ins Drinking Mo re He a vily Ca n’ t Pa y Re nt, Mo ve s to Stre e t I njury, Ca n’ t Wo rk Be g ins Wo rking a s Da y L a b o re r Mo ve s to Sa n F ra nc isc o I nflux o f Che a p US Co rn; Ca n’ t Ma ke a L iving 4th Ge ne ra tio n Co rn F a rme r in Oa xa c a I n E me rg e nc y De pa rtme nt Afte r F
Ge ts Assa ulte d Syste matic marginalization of and viole nc e against indige nous c ommunitie s in
Rac ialize d low-wage labor marke ts Be g ins Drinking Mo re He a vily Ca n’ t Pa y Re nt, Mo ve s to Stre e t I njury, Ca n’ t Wo rk Be g ins Wo rking a s Da y L a b o re r Mo ve s to Sa n F ra nc isc o I nflux o f Che a p US Co rn; Ca n’ t Ma ke a L iving 4th Ge ne ra tio n Co rn F a rme r in Oa xa c a I n E me rg e nc y De pa rtme nt Afte r F
Ge ts Assa ulte d Standar d Me dic al History & De fault Provide r Inte rpre tation
which structural violence is erased and elided by claims of cultural difference, genetic variance, behavioral shortcomings, or racial categories.
color)
realities
Nor th Ame r ic an F r e e T rade Agre e me nt (NAF T A) US immigr ation Polic y/ Disc rimination City polic ie s c ontributing to high re nts & displac e me nt No He alth Insuranc e Be g ins Drinking Mo re He a vily Ca n’ t Pa y Re nt, Mo ve s to Stre e t I njury, Ca n’ t Wo rk Be g ins Wo rking a s Da y L a b o re r Mo ve s to Sa n F ra nc isc o I nflux o f Che a p US Co rn; Ca n’ t Ma ke a L iving 4th Ge ne ra tio n Co rn F a rme r in Oa xa c a I n E me rg e nc y De pa rtme nt Afte r F
Ge ts Assa ulte d
a ffe c ting he a lth a nd he a lth c a re ?
In Emergency Department After Found on Street Begins Drinking More Heavily Gets Assaulted Can’t Pay Rent, Moves to Street Injury, Can’t Work Begins Working as Day Laborer Moves to San Francisco Influx of Cheap U.S. Corn Fourth Generation Corn Farmer in Oaxaca Educate yourself and work against implicit and explicit racism and other bias Approach the patient without blame
Use an interpreter Advocate for safe spaces for community members Research the structural forces that affect the lives and health of migrants who work as day laborers, including policy and racism in your research questions and discussion Advocate for more just housing policy Organize against trade agreements that contribute to the exploitation of foreign labor
Intrapersonal Interpersonal Clinic Community Research Policy
respond to health and illness as the downstream effects of broad social, political and economic structures
people of different cultures
health conditions, including mental health and substance use disorders
effectively and efficiently
Farmworkers: Final Report of the Indigenous Farmworker Study (IFS) to the California Endowment. Retrieved at http://www.indigenousfarmworkers.org
black disease. Beacon Press.
medical engagement with stigma and inequality. Social Science & Medicine, 103, 126-133.
violence and clinical medicine. PLoS medicine, 3(10), e449.