
SLIDE 1
HYPOXIC ISCHEMIC ENCEPHALOPATHY AND THE OBSTETRICIAN
Michael P. Nageotte, M.D.
DISCLOSURE
- I have nothing to disclose and have no real or
HYPOXIC ISCHEMIC ENCEPHALOPATHY AND I have nothing to disclose and - - PowerPoint PPT Presentation
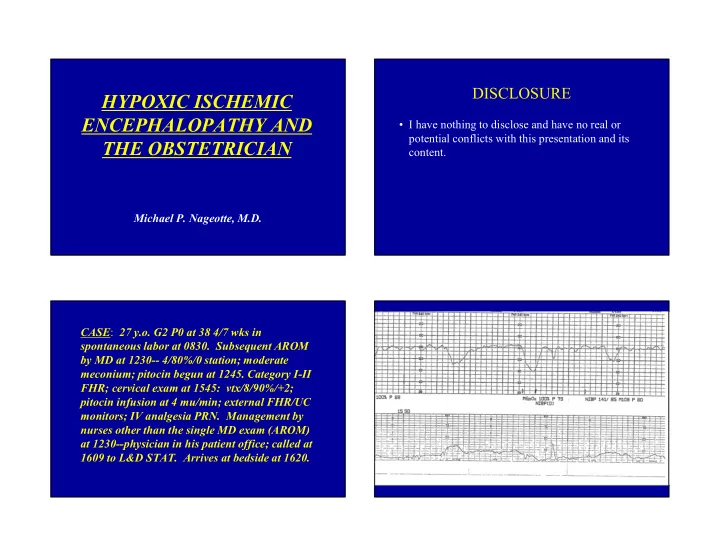
DISCLOSURE HYPOXIC ISCHEMIC ENCEPHALOPATHY AND I have nothing to disclose and have no real or potential conflicts with this presentation and its THE OBSTETRICIAN content. Michael P. Nageotte, M.D. CASE : 27 y.o. G2 P0 at 38 4/7 wks in
with skin incision at 1630 and delivery at 1632
meconium; Apgars 1/4/4 at one, five and ten minutes
and requiring intubation; Admit Dx: “Hypoxic Ischemic Encephalopathy”; transfer to Level III for total body cooling despite IUGR
Y e s N
18%
Hypoxia : Reduced amount of oxygen delivered to tissues;
encephalopathy or brain injury unlikely in the fetus or newborn
Hypoxemia: Reduced oxygen concentration in blood; associated
with hypoxia but injury unlikely if adequate cerebral blood flow
Hypoxia-Ischemia: Reduced oxygen and inadequate volume
intracellular oxygen and glucose remain below critical levels
Metabolic Acidosis: Low pH due to increased lactic acid in the
blood reflecting severity of asphyxia and/or hypoxia-ischemia
Respiratory Acidosis: Low pH due to increased carbon dioxide
in blood; may protect the fetal/neonatal brain due to reflex cerebral vasodilation and increased cerebral blood flow
Mixed Acidosis: Low pH reflecting both increased carbon
dioxide (respiratory) and lactic acid (metabolic); most common form of clinically significant neonatal acidosis
persists, to progressive hypoxemia and hypercapnia with a significant metabolic acidosis resulting (World Federation of Neurology, 1993)
duration rather than an endpoint and should not be applied to birth events unless specific evidence of markedly impaired intrapartum or immediate postnatal gas exchange can be linked to neurologic illness in the neonate (Low, 1997)
newborn and neonatal status have given rise to the term hypoxic ischemic encephalopathy (HIE)
perinatal asphyxia) describes a subset of NE present in the first week of life in term/near term infants believed to have experienced significant hypoxemia/asphyxia prior to or during labor and delivery
most severe state characterized by hypotonia, apnea/respiratory depression, coma and seizures
i n c r e a s e d d e c r e a s e d r e m a i n e d u n c h a n g e d
17% 80% 3%
Cerebral palsy describes a group of conditions specifically involving motor disability of early onset which, despite a wide range of possible abilities and disabilities, must satisfy the following: 1) motor disorder (specifically, spasticity, dyskinesia, ataxia, mixed or hypotonia) is present by age of four 2) cerebral not peripheral nerve or muscular abnormality 3) arises early in development 4) is not progressive or degenerative but life-long and with no known cure 5) may or may not be associated with other neurological
6) if fetal asphyxia is implicated, the CP must be of the spastic quadriparetic or dyskinetic type
cognition, speech, epilepsy and behavioral disorders
likely that a number of these impairments will add to the complexity of the disorder.
generally a more severe form with milder CP evident
age at birth decreases with < 32 weeks gestation being the strongest risk factor for CP.
steadily since the mid 1990s, this has had little impact
comprise only 2% of all births.
yet comprise 60% of CP cases (term/late preterm neonates account for 98% of all births).
the rate of 2/1000 consistent throughout the developed world for the past several decades.
to hypoxia-ischemia, with specific MRI established abnormalities, following a recognized obstetrical sentinel event (e.g. uterine rupture, cord prolapse, maternal cardiac arrest).
the accepted cause of encephalopathy but not all sentinel events result in HIE and one cannot implicate hypoxia-ischemia with 100% certainty because it is not possible to document blood flow and oxygenation of the fetal brain.
different from hypoxia-ischemia is identified (e.g. trauma, infection or specific metabolic disorder).
conundrum as there is a lack of an obvious cause of the neurologic abnormalities identified.
mind in all cases and a clear history of hypoxia- ischemia associated with a sentinel event does not rule
Myers, 1972, 1975)
dysplasia to focal infarcts and atrophy or basal ganglion lesions (related to insult timing/severity)
basal ganglia, thalamus and periphery of the cerebral cortex
1) Selective neuronal necrosis of the cortex,
T r u e F a l s e
91% 9%
(Yudkin PL, Ped Perinatal Epidemiol 1988; 156:170)
(N=164; Controls=400)
2.55 1.3-4.9
2.73 1.2-6.4
4.43 1.1-17.6
9.7 2.0-47.9
6.3 2.3-17.7
3.6 1.3-9.9
3.0 1.5-5.8
2.97 1.2-3.7
38.2 9.4-154.8
13.2 5.0-34.8 (Badawi, N, et al 1998;BMJ 317:1554)
O.R. 95% C.I.
(Badawi, N, et al 1998;BMJ 317:1554)
(Badawi, N, et al 1998;BMJ 317:1554)
O.R. 95% C.I.
(Wu, Yvonne; Editorial, Annals of Neurology 2012 V.72: 151-2)
30% of cases of neonatal encephalopathy.
associated with clear intrapartum hypoxia-ischemia.
including those who meet the clinical and MRI criteria for HIE, the exact mechanism and timing of brain injury remains unknown and unknowable.
do not know and we do not know how to prevent neonatal brain injury.
preterm, multiples or depressed neonates
communication among all health care providers
before discharge to assess nature and general timing of injury with interpretation by skilled neuroradiologists
ischemia from diminished blood flow usually but not necessarily preceded or accompanied by hypoxemia (diminished amount of oxygen in the blood supply)
myocardial disturbance leading to the critically important loss of CNS vascular autoregulation resulting in ischemia (hypoperfusion injury)
as the gestational age, presence of co-morbidities and potentially preceding events strongly influence the presence and degree of resultant neuropathology
reduced that oxygen content of the blood delivered to the brain is below the level needed to avoid energy failure in brain cells; metabolism is disturbed, neuronal cell integrity is not maintained and cellular injury, dysfunction or neuronal cell death results.
CNS are not available in current clinical settings.
biomarkers, EFM, scalp/umbilical artery pH, etc.
lesions establishes timing, severity and etiology remains open to debate as sentinel events are not always followed by specific MRI abnormalities.
typically noted in the periventricular white matter, the region with the most tenuous perfusion, sparing the subcortical white matter and cortex
in the mature intervascular boundary zones (“watershed”) which include the periventricular white matter, subcortical white matter and cerebral cortex in the boundary regions. The deep gray matter structures
finding (ultrasound or MRI) of preterm fetuses at risk for CP from in utero/intrapartum/perinatal injury
damages nearly the entire brain with no useful patterns detected by any modality of imaging.
that vary with the state of brain maturity.
in injury primarily to the lateral thalami.
and perirolandic cortex may be injured.
from the internal capsule to the perirolandic cortex within the basal ganglia (likely due to the higher metabolic activity in these areas of the brain).
0.00% 20.00% 40.00% 60.00% 80.00% 100.00% Cases Controls 5 M in Apgar <3 5 M in Apgar 3-6 5 M in Apgar >6
(Badawi, N, et al 1998;BMJ 317:1554)
O.R. 95% C.I.
(Badawi, N, et al 1998;BMJ 317:1554)
– Spontaneous Vag 1.0 1.0 – Elective C/S 0.17 0.05-0.56
(Badawi, N, et al 1998;BMJ 317:1554)
O.R. C.I.
6527 6552
12 (.018%) 27(.041%)*
3 (.005%) 6(.009%)
21(.032%)
3(0.005%) 3(0.005%)
12 (.018%) 10(.015%) EFM I.A. (Grant A, Lancet: Nov. 25, 1989)