
SLIDE 1
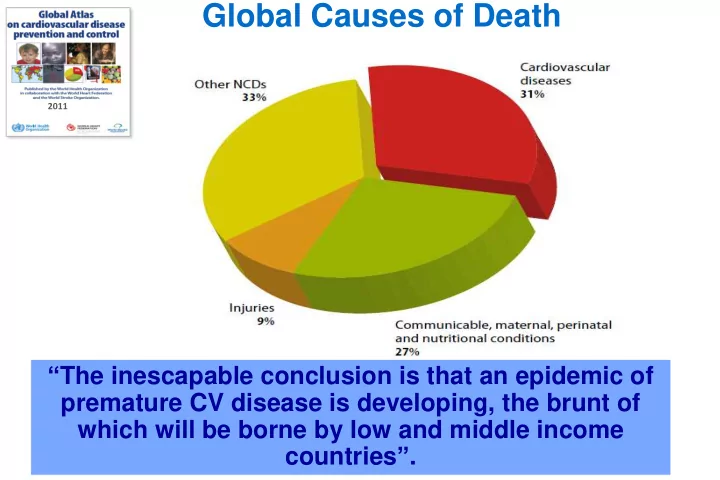
Global Causes of Death
- NCDs cause 64% (35 million) of global deaths
- 80% (28 million) are in LMICs
- NCDs will cost the world $47 trillion over the next 20 years
- CVD is responsible for around one third of all deaths worldwide
2011
“The inescapable conclusion is that an epidemic of premature CV disease is developing, the brunt of which will be borne by low and middle income countries”.