
SLIDE 1
EXPANDED CARRIER SCREENING
Mary E Norton MD University of California, San Francisco
OBGYN Update UCSF, San Francisco CA 2019
Disclosures
- Research funding from Natera
- Consultant to Invitae
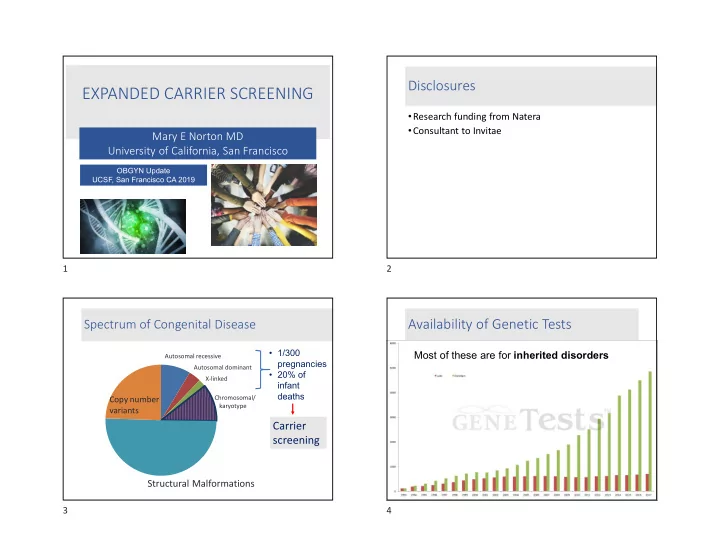
Spectrum of Congenital Disease
Structural Malformations
Autosomal recessive Autosomal dominant X-linked Chromosomal/ karyotype
Copy number variants
- 1/300
pregnancies
- 20% of