
SLIDE 1
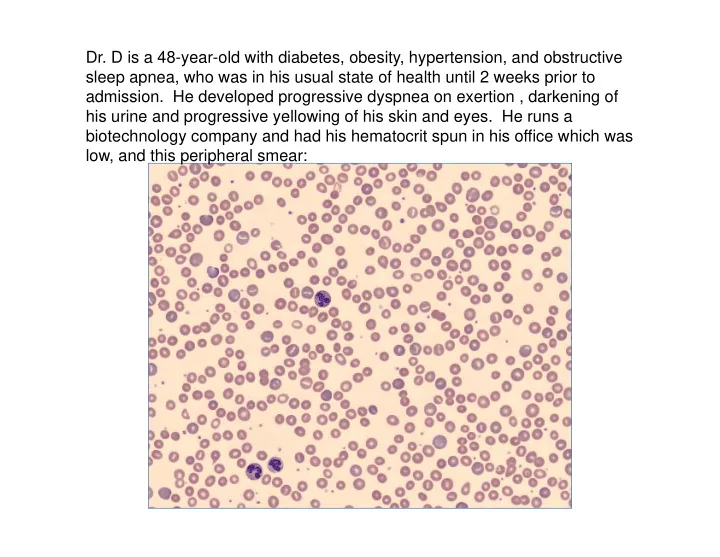
- Dr. D is a 48-year-old with diabetes, obesity, hypertension, and obstructive
sleep apnea, who was in his usual state of health until 2 weeks prior to
- admission. He developed progressive dyspnea on exertion , darkening of
his urine and progressive yellowing of his skin and eyes. He runs a biotechnology company and had his hematocrit spun in his office which was low, and this peripheral smear: