
SLIDE 1
2/14/2019 1
Deep Brain Stimulation for Multiple Movement Disorders
Jill Ostrem, MD Carlin and Ellen Wiegner Endowed Professor of Neurology Division Chief and Medical Director UCSF Movement Disorder and Neuromodulation Center
Disclosures
- Consultant: AbbVie, Adamas, Neurocrine, Acadia
- Educational grant support: Medtronic, Allergan, Boston
Scientific, AbbVie
- Clinical trial support: Boston Scientific, Cala Health, Medtronic,
Biogen
DBS for Movement Disorders
Approved indications:
- Essential tremor
- Parkinson’s disease
- Isolated dystonia
Off label indications:
- Tardive dystonia
- Secondary dystonia
- Tourette syndrome
- Orthostatic tremor
- Holmes tremor
- Musician’s dystonia
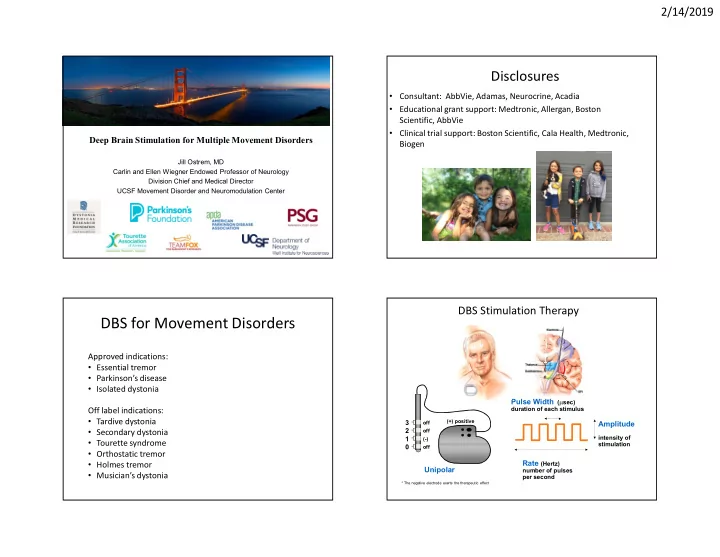
DBS Stimulation Therapy
* The negative electrode exerts the therapeutic effect
Unipolar
1 2 3
- ff
- ff
(-)
- ff
(+) positive
Rate (Hertz)
number of pulses per second
Pulse Width (sec)
duration of each stimulus
Amplitude
intensity of stimulation