
SLIDE 1
12/8/19 1
Should We Ablate Asymptomatic AF in a Young Patient? Pro
Edward Paul Gerstenfeld, MD, FHRS
@Ed_Gerst
Professor of Medicine University of California, San Francisco 2.0
1
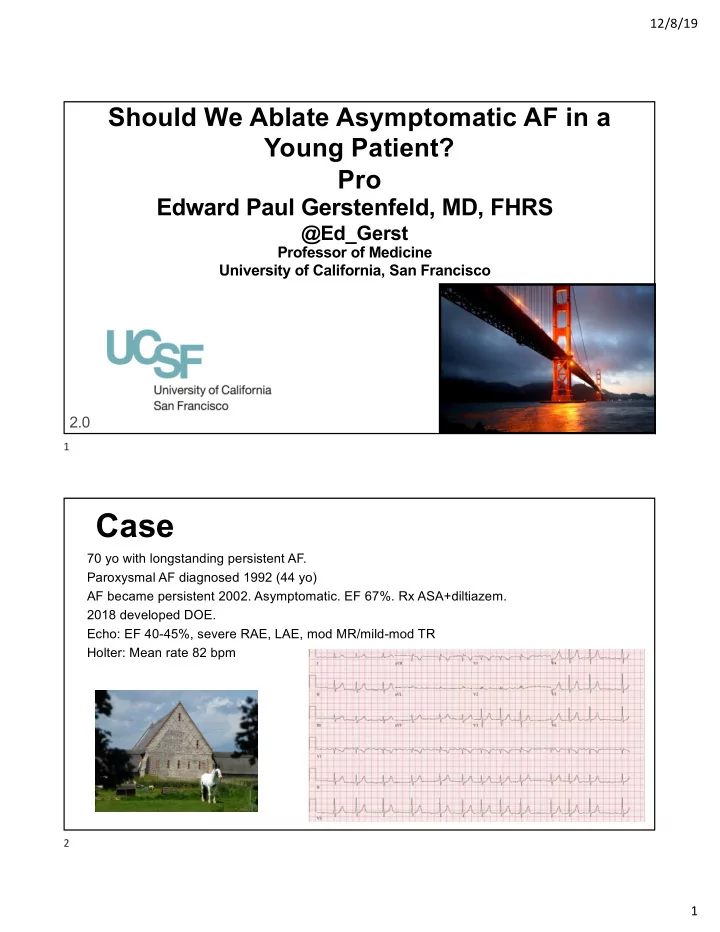
70 yo with longstanding persistent AF. Paroxysmal AF diagnosed 1992 (44 yo) AF became persistent 2002. Asymptomatic. EF 67%. Rx ASA+diltiazem. 2018 developed DOE. Echo: EF 40-45%, severe RAE, LAE, mod MR/mild-mod TR Holter: Mean rate 82 bpm
Case
2