
SLIDE 1
5/26/2017 1 Pitfalls in Gastrointestinal and Hepatic Pathology
Laura W. Lamps M.D. Godfrey D. Stobbe Professor of Gastrointestinal Pathology University of Michigan Department of Pathology Patient Safety Officer, Michigan Medicine Ann Arbor, MI
- Unforced error (LWL)
– A player makes an error that is not the result of an action by his/her opponent – The player has full control of his/her actions, but still makes a mistake
- Forced error (LWL plus clinician)
– The opponent hits a difficult shot and causes the player to miss – Succumbing to an impossible ball that can’t be returned
- Errors from the stands
– Errors that I did not actually commit, but watched happen, and had good seats
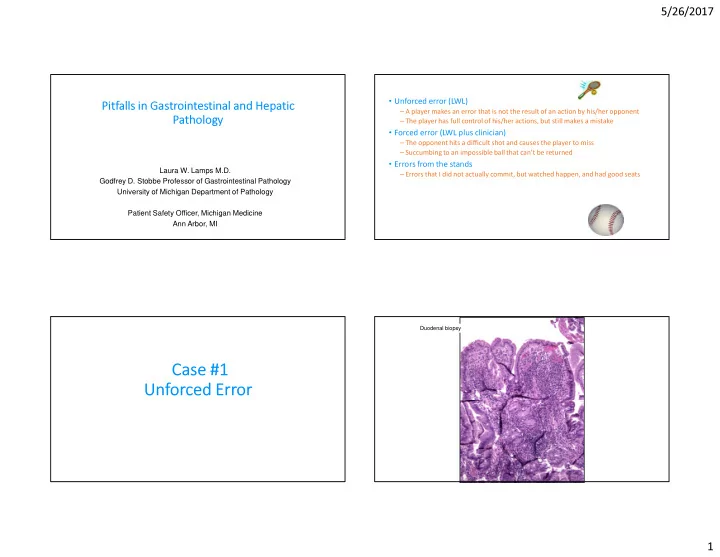
Case #1 Unforced Error
50 year old woman s/p renal transplant, with diarrhea
Duodenal biopsy