
SLIDE 1
An eroded lesion in either the esophageal, gastric, or duodenal - - PowerPoint PPT Presentation
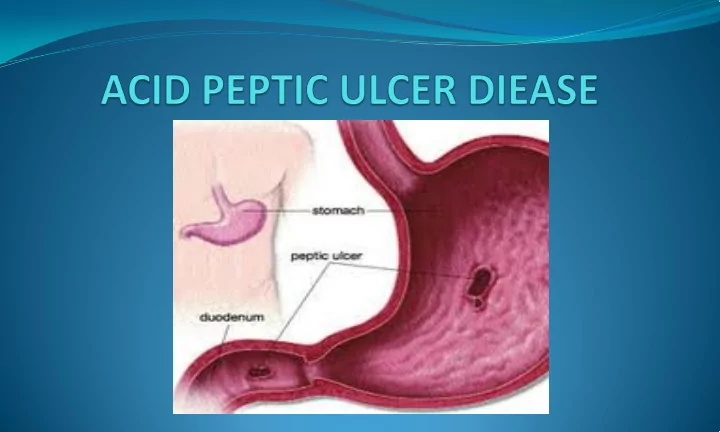
An eroded lesion in either the esophageal, gastric, or duodenal mucosa resulting from the action of gastric secretions and typically H.pulori bacterial inflammation. Normal gastric and duodenal mucosa is protected from the digestive actions