
SLIDE 1
Aging, Dementia, and Developmental Disabilities March 3, 2016 Seth M. - - PDF document
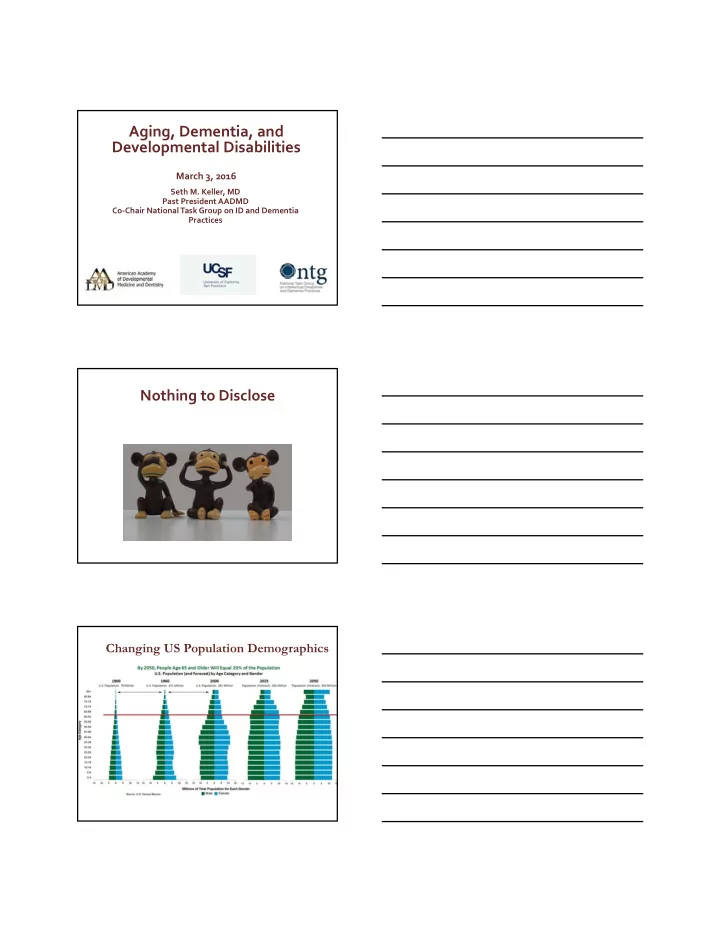
Aging, Dementia, and Developmental Disabilities March 3, 2016 Seth M. Keller, MD Past President AADMD Co Chair National Task Group on ID and Dementia Practices Nothing to Disclose Changing US Population Demographics Aging and Intellectual and
Carter & Jancar, 1983, Janicki, Dalton, Henderson, & Davidson, 1999
Curr Gerontol Geriatr Res. 2012; 2012: 412-536.
Rubin & Crocker,2006; Yang Rasmussen & Friedman, 2002
▪ Osteopenia/Osteoporosis ‐ normal aging‐related bone loss ▪ Sarcopenia ‐ progressive loss of muscle mass ▪ Presbyopia: the lens of the eye becomes stiffer and less flexible – affecting the
ability to focus on close objects (accommodation)
▪ Presbycusis – aging related change in the ability to detect higher pitches –
more noticeable in those age 50+
▪ Gustation (i.e. the sense of taste) decrements become more noticeable
beyond 60+
▪ Olfaction (i.e. the sense of smell), decrements become more noticeable after
age 70+
▪ Somatosensory System ‐ Reduction in sensitivity to pain, touch, temperature,
proprioception
▪ Vestibular – Reduction in balance and coordination ▪ Cognitive – Reduction in short term memory loss, attention, and, retrieval
Susceptibility to disease Individual organ systems age differently Social and cultural factors Compensatory behaviors + access to resources Lifestyle Genetic predisposition
Baltes, P. B., & Baltes, M. M. (1990). Psychological perspectives on successful aging: The model of selective optimization with compensation. In P. B. Baltes & M. M. Baltes (Eds.), Successful aging: Perspectives from the behavioral sciences (pp. 1–34). New York: Cambridge University Press
Rowe, J. W., & Kahn, R. L. (1997). Successful
9
supplements)
bearing exercises)
with people)
1 Heart disease 2 Cancer 3 Chronic lower respiratory diseases 4 Stroke 5 Alzheimer’s disease 6 Diabetes 7 Influenza and pneumonia 8 Kidney disease 9 Accidents (unintentional injuries) 10 Septicemia
13
Heron M. Deaths: Leading causes for 2010. National vital statistics reports; vol 62 no 6. Hyattsville, MD: National Center for Health
▪ Prader‐Willi syndrome
▪ Psychosis and behavioral changes ▪ Obesity‐related adverse
▪ Williams syndrome
▪ Premature memory loss ▪ Problems in multiple organ
systems
▪ Fragile X syndrome
▪ Fragile X‐associated
tremor/ataxia syndrome (FXTAS)
▪ Down syndrome
▪ Premature aging ▪ Early onset dementia
▪ Autism spectrum disorders
▪ Mental health aspects
(depression, etc.)
▪ Medication effects (long
term)
▪ Cerebral palsy
▪ Deconditioning ▪ Cervical spondylotic
myelopathy
▪ Pain ▪ Osteoporosis ▪ GI & GU issues
▪ Immediate recall, word finding, or complex problem solving
problems (½ of these folks will develop dementia in 5 yrs)
(seek medical help immediately )
know”, “I just can’t” responses, no pleasure can look like agitation & confusion
Source: Diagnostic and Statistical Manual of Mental
Alzheimer’s Disease
Vascular Dementias (Multi-infarct) Lewy Body Dementia
Other Dementias
Mental conditions
Fronto- Temporal Lobe Dementias
(1864-1915) Auguste Deter
1 2 3 4 5 6 7 8 9 5 10 15 20 25 30 Time (years) Symptoms Diagnosis Loss of functional independence Behavioural problems
Specialized supportive care
Death Mini-Mental State Examination (MMSE)
Feldman and Gracon. The Natural History of Alzheimer’s Disease. London: Martin Dunitz, 1996
Percentage of people with Down syndrome who develop dementia at different ages: Age percentage with clinical signs
30’s 2% 40’s 10‐15% 50’s 33% 60’s 50‐70%
Source: Neil, M. (2007). Alzheimer's dementia: What you need to know, what you need to do. Understanding intellectual disability and health. Accessed from http://www.intellectualdisability.info/mental‐ health/alzheimers‐dementia‐what‐you‐need‐to‐know‐what‐ you‐need‐to‐do.
Fraser, J, Mitchell, A., (1876). Kalmuc idiocy: report of a case with autopsy with notes on 62 cases. Journal of Mental Science 22, 161. Jervis, GA. Early senile dementia in mongoloid idiocy. (1948) The American Journal of Psychiatry, 105, 102-106. Oliver, C., Holland, AJ (1986) Down Syndrome and Alzheimer’s disease: a review. Psychological Medicine 16, 307-22.
Percent persons with Down syndrome showing evidence of neurofibrillary tangles (NFT) and senile plaques (SP) at autopsy Nelson, L. D. et al. Arch Neurol 2011;68:768‐774.
Representative Amyloid Scans in DS and AD
Mann, D.M.A. (1993). Association between Alzheimer disease and Down syndrome: Neuropathological
(Eds.),Alzheimer disease and Down syndrome and their relationship (pp. 71-92). Oxford University Press
Seth M Keller, MD Matthew P. Janicki, PhD NTG Co‐Chairs sethkeller@aol.com mjanicki@uic.edu http://aadmd.org/ntg