SLIDE 1 Abstract Session A4: Clinical Epidemiology/Healthcare Effectiveness Research
Moderator: Howard S. Gordon, MD
FOOD INSECURITY IS ASSOCIATED WITH DIABETES SELF-CARE BEHAVIORS AND GLYCEMIC CONTROL William J. Heerman1; Ken Wallston2; Chandra Y. Osborn3; David Schlundt4; Shari D. Barto1; Russell L. Rothman1. 1Vanderbilt University Medical Center, Nashville, TN; 2Vanderbilt University Medical Center, Nashville, TN; 3Vanderbilt University Medical Center, Nashville, TN; 4Vanderbilt University, Nashville, TN. (Tracking ID #1928444) BACKGROUND: Food insecurity is the "limited or uncertain availability of nutritionally adequate and safe foods," and has been associated with worse glycemic control among patients with type 2 diabetes (T2DM). Less is known about food insecurity's relationship with diabetes self-care behaviors, and whether its effects on glycemic control can be attributed to that relationship. Therefore, we examined the relationships between food insecurity, self-care, and glycemic control, and whether any effect on glycemic control was due to relationships with self-care. METHODS: We conducted a cross-sectional analysis of baseline data from patients with T2DM enrolled in a randomized trial evaluating a health literacy-focused diabetes intervention at 10 county health departments across middle Tennessee. Food insecurity was assessed with 3 items from the U.S. Household Food Security Survey and patients who answered "sometimes" or "often" to at least one of these items were considered "food insecure." Diabetes self-care behaviors were assessed with the Summary of Diabetes Self Care Activities Scale (SDSCA), Personal Diabetes Questionnaire (PDQ-11), and Adherence to Refills and Medication Scale (ARMS). Glycemic control was assessed with A1C, collected prospectively unless available in medical record within 4 weeks of study
- enrollment. Student's t-tests or Wilcoxon rank-sum tests were used to evaluate the bivariate relationships between food insecurity and
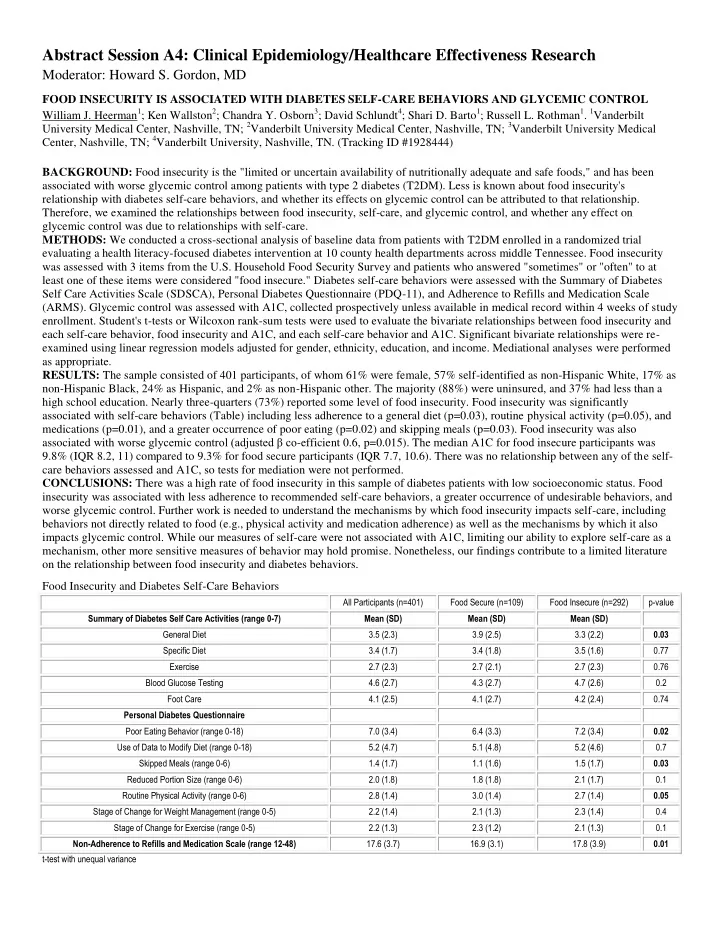
each self-care behavior, food insecurity and A1C, and each self-care behavior and A1C. Significant bivariate relationships were re- examined using linear regression models adjusted for gender, ethnicity, education, and income. Mediational analyses were performed as appropriate. RESULTS: The sample consisted of 401 participants, of whom 61% were female, 57% self-identified as non-Hispanic White, 17% as non-Hispanic Black, 24% as Hispanic, and 2% as non-Hispanic other. The majority (88%) were uninsured, and 37% had less than a high school education. Nearly three-quarters (73%) reported some level of food insecurity. Food insecurity was significantly associated with self-care behaviors (Table) including less adherence to a general diet (p=0.03), routine physical activity (p=0.05), and medications (p=0.01), and a greater occurrence of poor eating (p=0.02) and skipping meals (p=0.03). Food insecurity was also associated with worse glycemic control (adjusted β co-efficient 0.6, p=0.015). The median A1C for food insecure participants was 9.8% (IQR 8.2, 11) compared to 9.3% for food secure participants (IQR 7.7, 10.6). There was no relationship between any of the self- care behaviors assessed and A1C, so tests for mediation were not performed. CONCLUSIONS: There was a high rate of food insecurity in this sample of diabetes patients with low socioeconomic status. Food insecurity was associated with less adherence to recommended self-care behaviors, a greater occurrence of undesirable behaviors, and worse glycemic control. Further work is needed to understand the mechanisms by which food insecurity impacts self-care, including behaviors not directly related to food (e.g., physical activity and medication adherence) as well as the mechanisms by which it also impacts glycemic control. While our measures of self-care were not associated with A1C, limiting our ability to explore self-care as a mechanism, other more sensitive measures of behavior may hold promise. Nonetheless, our findings contribute to a limited literature
- n the relationship between food insecurity and diabetes behaviors.
Food Insecurity and Diabetes Self-Care Behaviors
All Participants (n=401) Food Secure (n=109) Food Insecure (n=292) p-value Summary of Diabetes Self Care Activities (range 0-7) Mean (SD) Mean (SD) Mean (SD) General Diet 3.5 (2.3) 3.9 (2.5) 3.3 (2.2) 0.03 Specific Diet 3.4 (1.7) 3.4 (1.8) 3.5 (1.6) 0.77 Exercise 2.7 (2.3) 2.7 (2.1) 2.7 (2.3) 0.76 Blood Glucose Testing 4.6 (2.7) 4.3 (2.7) 4.7 (2.6) 0.2 Foot Care 4.1 (2.5) 4.1 (2.7) 4.2 (2.4) 0.74 Personal Diabetes Questionnaire Poor Eating Behavior (range 0-18) 7.0 (3.4) 6.4 (3.3) 7.2 (3.4) 0.02 Use of Data to Modify Diet (range 0-18) 5.2 (4.7) 5.1 (4.8) 5.2 (4.6) 0.7 Skipped Meals (range 0-6) 1.4 (1.7) 1.1 (1.6) 1.5 (1.7) 0.03 Reduced Portion Size (range 0-6) 2.0 (1.8) 1.8 (1.8) 2.1 (1.7) 0.1 Routine Physical Activity (range 0-6) 2.8 (1.4) 3.0 (1.4) 2.7 (1.4) 0.05 Stage of Change for Weight Management (range 0-5) 2.2 (1.4) 2.1 (1.3) 2.3 (1.4) 0.4 Stage of Change for Exercise (range 0-5) 2.2 (1.3) 2.3 (1.2) 2.1 (1.3) 0.1 Non-Adherence to Refills and Medication Scale (range 12-48) 17.6 (3.7) 16.9 (3.1) 17.8 (3.9) 0.01 t-test with unequal variance
SLIDE 2
COMPARATIVE EFFECTIVENESS OF A PRACTICE-BASED TRIAL OF BLOOD PRESSURE CONTROL IN BLACKS: IS LESS MORE? Antoinette Schoenthaler1; Jeanne Teresi2; Leanne Luerassi1; Stephanie Silver2; Jian Kong2; Taiye Odedosu1; Gbenga Ogedegbe1. 1New York University School of Medicine, New York, NY; 2The Hebrew Home at Riverdale, Riverdale, NY. (Tracking ID #1929818) BACKGROUND: The efficacy of interventions targeted at comprehensive therapeutic lifestyle changes (TLC) is well proven in reducing blood pressure (BP) among patients with hypertension (HTN). However their translation to primary care practices is limited, particularly among black patients with HTN, who share a disproportionately greater burden of HTN-related outcomes. More importantly, the comparative effectiveness of single session TLC interventions on BP reduction in primary care practices is unproven. The aim of this vanguard trial was to evaluate the comparative effectiveness of a practice-based comprehensive lifestyle intervention targeted at recommended TLC, delivered through group-based counseling and motivational interviewing (MINT), versus a single session counseling on lifestyle modification (SSC) in reducing BP at six months among low-income, blacks with uncontrolled HTN. METHODS: A total of 194 black patients were randomized to either the MINT-TLC or SSC group. The comprehensive lifestyle intervention (MINT-TLC) was based on established clinical practice guidelines for prevention and treatment of HTN, which recommends weight loss (if overweight), regular physical activity, limiting and/or reducing sodium and alcohol intake, and eating a low-fat diet that is rich in fruit and vegetables. Patients in the MINT-TLC group attended 10 weekly group classes (intensive phase) focused on TLC; followed by 3 monthly individual MINT sessions (maintenance phase) delivered by trained Health Educators. Patients in the SSC condition received a single 30-minute individual counseling session on therapeutic lifestyle changes at the baseline visit by trained study staff. To match the MINT-TLC group for content of intervention material, those in the SSC group also received print versions of the intervention curriculum that was distributed in the group classes. The primary outcome was change in systolic BP and diastolic BP at 6 months assessed with an automated BP monitor (WatchBP). The average of three BP readings was used as the primary outcome measurement, following standard American Heart Association guidelines. The primary analyses examined systolic and diastolic BP separately based on intent-to-treat. A repeated measures mixed model approach was used to account for continuous primary outcomes collected at three waves (baseline, 3 and 6 months), and clustering within primary care providers. The post-treatment values of continuous outcomes were modeled as functions of baseline values, treatment and the interaction of baseline and treatment. RESULTS: The mean age of all patients was 57 years, 50% were women, 69% had income < $20,000/year with mean baseline BP 147.4/89.3 mmHg. Average attendance at the group-based classes in the MINT-TLC condition was 50%; 35% of patients completed all 3 individual MINT sessions. There was non-significant reduction in systolic and diastolic BP for the MINT-TLC compared to the SSC group. The net adjusted reduction in systolic BP by six months was 12.9 mmHg for the SSC vs. 9.5 mmHg for the MINT-TLC group. The reduction in diastolic BP was 7.6 mmHg for the SSC vs. 7.2 mmHg for the MINT-TLC group. CONCLUSIONS: Despite the non-significant between-group difference in BP reduction in the intensive group counseling with multiple office visits versus the single counseling session plus educational material both groups exhibited comparable and clinically meaningful BP reduction. Evaluation of the effectiveness of the interventions in a large Phase 3 trial is warranted in this patient population. Trial Registration: Clinicaltrials.gov NCT01070056
SLIDE 3 SUBCLINICAL THYROID DYSFUNCTION AND FRACTURE RISK: AN INDIVIDUAL PARTICIPANT DATA ANALYSIS OF PROSPECTIVE COHORTS
Manuel R. Blum1; Douglas Bauer2; Bruno R. da Costa3; Christina D. Wirth1; Anne R.Cappola4; Robin P. Peeters5; Bjørn O. Åsvold6; Howard A. Fink7,8; Wendy P. den Elzen9; Robert N. Luben10; Misa Imaizumi11; Arnulf Langhammer6; Alexandra P. Bremner12; Apostolos Gogakos13; Richard Eastell14; Elsa S. Strotmeyer15; Erin Wallace16; Mari Hoff6,17; Kay-Tee Khaw10; Graziano Ceresini18; Fernando Rivadeneira5; Luigi Ferrucci19; André Uitterlinden5; Graham R. Williams13; Rudi G. Westendorp20; John P. Walsh21,22; Jacobijn Gussekloo9; Drahomir Aujesky1; Nicolas Rodondi1.
1Inselspital, Bern University Hospital, Bern, Switzerland; 2University of California, San Francisco, CA; 3University of Bern, Bern, Switzerland; 4University of Pennsylvania School of Medicine, Philadelphia, PA; 5University of Rotterdam, Rotterdam, Netherlands; 6Norwegian University of
Science and Technology, Trondheim, Norway; 7University of Minnesota School of Medicine, Minneapolis, MN; 8VA Medical Center, Minneapolis, MN;
9Leiden University Medical Center, Leiden, Netherlands; 10University of Cambridge, Cambridge, United Kingdom; 11Radiation Effects Research
Foundation, Nagasaki, Japan; 12University of Western Australia, Crawley, WA, Australia; 13Imperial College London, London, United Kingdom;
14University of Sheffield, Sheffield, United Kingdom; 15University of Pittsburgh, Pittsburgh, PA; 16University of Washington, Seattle, WA; 17Nord-
Trøndelag Hospital Trust, Levanger, Norway; 18University Hospital of Parma, Parma, Italy; 19National Institute on Aging, National Institutes of Health, Baltimore, MD; 20Leiden University Medical Center, Leiden, Netherlands; 21University of Western Australia, Crawley, WA, Australia; 22Sir Charles Gairdner Hospital, Nedlands, WA, Australia. (Tracking ID #1930001) BACKGROUND: Subclinical thyroid dysfunction is common, particularly with increasing age. Controversy persists as to whether screening and treatment of subclinical thyroid dysfunction are warranted, as current evidence about the risks and effects of treatment is
- limited. Data from several prospective cohorts on the association between subclinical thyroid dysfunction and fracture events are
- conflicting. These conflicting results might be attributed to differences in age, gender, thyrotropin (TSH) levels, power and varying
cut-offs of the studies. METHODS: After a systematic literature review, we performed an individual participant pooled data analysis from all available prospective cohorts of adults with measurement of baseline thyroid function and fracture outcomes. We examined hip, non-spine, clinical spine and any fractures. We defined euthyroidism as TSH 0.45-4.49 mIU/L, subclinical hyperthyroidism as TSH<0.45 mIU/L with normal free thyroxine (FT4) levels and subclinical hypothyroidism as TSH≥4.50-19.99 mIU/L with normal FT4 levels. RESULTS: Among 13 prospective cohort studies with 69,795 participants during 757,219 person-years of follow-up, 4044 (5.8%) participants had subclinical hypothyroidism and 2091 (3.0%) had subclinical hyperthyroidism. During follow-up, 2901 participants (among 12 studies) had a hip fracture, 2018 (8 studies) had non-spine fractures, 320 (7 studies) had spine-fractures, and 2600 (9 studies) had any fracture. In age and gender-adjusted analyses, the overall hazard ratio (HR) for individuals with subclinical hyperthyroidism of any cause compared to euthyroidism was 1.39 (95% confidence interval, 1.10-1.76) for hip fracture, 1.16 (0.95- 1.41) for non-spine fracture, 1.54 (0.96-2.47) for spine fracture, and 1.28 (1.07-1.54) for any fracture. The risk of fracture increased with lower TSH levels for every fracture outcome (all p for trend≤0.02). Compared to euthyroid participants, HRs for those with TSH<0.10 mIU/L were 1.67 (1.21-2.30) for hip fracture, 1.72 (1.11-2.68) for non-spine fracture, 3.57 (1.88-6.78) for spine fracture, and 2.01 (1.49-2.71) for any fracture. Risks were similar after further adjustment for known osteoporotic fracture risk factors such as BMI and smoking. The attributable risk for subclinical hyperthyroidism was 28% for hip fracture and 22% for any fracture. Endogenous subclinical hyperthyroidism (no use of thyroid hormone) was associated with increased fracture risk for all fracture
- utcomes, with HR of 1.56 (1.20-2.02) for hip, 1.27 (1.02-1.59) for non-spine, 1.74 (1.01-2.99) for spine and 1.42 (1.16-1.74) for any
- fracture. Subclinical hypothyroidism was not associated with fracture risk. HRs for participants on thyroid medication (N=2737) vs.
untreated euthyroid participants were 1.36 (1.15-1.61) for hip, 1.31 (1.08-1.59) non-spine, 1.34 (0.87-2.07) for spine and 1.24 (1.04- 1.47) for any fracture. CONCLUSIONS: Pooled individual data from 13 prospective cohorts confirm that subclinical hyperthyroidism is associated with an increased risk of hip and other fractures, particularly in those with a TSH concentration <0.10 mIU/L. Subclinical hypothyroidism is not associated with fracture risk, but treatment with thyroxine is associated with increased fracture risk. Our study cannot address whether treatment of subclinical hyperthyroidism reduces fracture risk, but our results indicate that trials of subclinical hyperthyroidism treatment are needed to identify optimal management strategies in these individuals.
Age and gender-adjusted risks associated with subclinical hyperthyroidism (vs. euthyroidism)
participants TSH <0.45 mIU/L vs. euthyroidism: HR (95% CI) TSH 0.10-0.44 vs. euthyroidism: HR (95% CI) TSH <0.10 vs. euthyroidism: HR (95% CI) P for trend * Hip fracture 2'616 / 58'106 1.39 (1.10-1.76) 1.37 (0.99-1.90) 1.67 (1.21-2.30) 0.002 Non-spine fracture 1'846 / 22'651 1.16 (0.95-1.41) 1.03 (0.81-1.30) 1.72 (1.11-2.68) 0.02 Clinical spine fracture 292 / 21'312 1.54 (0.96-2.47) 1.19 (0.65-2.20) 3.57 (1.88-6.78) < 0.001 Any fracture 2'378 / 27'041 1.28 (1.07-1.54) 1.11 (0.89-1.39) 2.01 (1.49-2.71) < 0.001
CI, confidence interval; HR, hazard ratio; TSH, thyroidea-stimulating hormone * P for trend across TSH categories (euthyroidism 0.45-4.49 mIU/L, TSH 0.10-0.44 mIU/L, and TSH <0.10 mIU/L)
SLIDE 4
AZITHROMYCIN IS ASSOCIATED WITH INCREASED CARDIAC EVENTS BUT LOWER MORTALITY FOR OLDER PATIENTS HOSPITALIZED WITH PNEUMONIA Eric Mortensen1,2; Ethan Halm2; Michael J. Fine3; Christopher Johnson1,2; Antonio Anuzeto4. 1VANTHCS, Dallas, TX; 2University of Texas Southwestern Medical Center, Dallas, TX; 3VA Pittsburgh Health Care System, Pittsburgh, PA; 4South Texas Veterans Health Care System, San Antonio, TX. (Tracking ID #1931222) BACKGROUND: Although clinical practice guidelines recommend combination therapy with macrolides, including azithromycin, as first line therapy for patients hospitalized with pneumonia, recent research suggests that azithromycin may be associated with increased cardiovascular events. The purpose of this study was to examine the association of azithromycin use with all-cause mortality and cardiovascular events for patients hospitalized with pneumonia. METHODS: We conducted a retrospective national study using Department of Veterans Affairs administrative data of patients hospitalized at any Veterans Administration acute care hospital. We included patients >65 years hospitalized with pneumonia in fiscal years 2002-2012. We included only those who received antibiotic therapy concordant with national clinical practice guidelines. Our outcomes included all-cause mortality, cardiac arrhythmias, heart failure, myocardial infarction, and any cardiac event. We used propensity score matching to control for the possible effects of known confounders with conditional logistic regression. RESULTS: Out of the 77,972 patients identified, our propensity-matched groups were composed of 34,763 azithromycin-exposed and 34,763 matched unexposed. There were no significant differences in potential confounders between groups after matching. We found that 90-day mortality was significantly lower in those who received azithromycin (exposed- 17.4% vs. unexposed- 22.8%, odds ratio [OR] 0.71, 95% confidence interval [CI] 0.68-0.73). However, we found significant increased odds of any cardiac event (43.2% vs 42.2%, OR 1.04, 95% CI 1.01-1.07), myocardial infarctions (4.9% vs. 4.2%, OR 1.17, 95% CI 1.09-1.26), and cardiac arrhythmias (26.5% vs. 25.6%, OR 1.04, 95% CI 1.002-1.07) but not heart failure (26.1% vs. 25.8%, OR 1.02, 95% CI 0.98-1.05). CONCLUSIONS: In patients hospitalized with pneumonia we found that although azithromycin is associated with a small increase in cardiac events it is also associated with a significant decrease in all-cause mortality. Our study supports the current clinical practice guidelines that recommend the use of azithromycin as part of empiric combination therapy.
SLIDE 5 EVALUATION OF STEPPED CARE FOR CHRONIC PAIN (ESCAPE) IN VETERANS OF IRAQ AND AFGHANISTAN: A RANDOMIZED TRIAL Matthew J. Bair1,2; Dennis Ang4; Jingwei Wu5; Samantha D. Outcalt1; Christy Sargent1; Amanda Gerwig1; Arlene Schmid6; Teresa Damush1,3; Zhangsheng Yu5; Louanne W. Davis7; Kurt Kroenke1,3. 1VA HSR&D Center for Health Information and Communication, Indianapolis, IN; 2Indiana University School of Medicine, Indianapolis, IN; 3Regenstrief Institute, Inc, Indianapolis, IN; 4Wake Forest School of Medicine, Winston- Salem, NC; 5Indiana University School of Medicine, Indianapolis, IN; 6Colorado State University, Fort Collins, CO; 7Roudebush VA Medical Center, Indianaplis, IN. (Tracking ID #1937595) BACKGROUND: Despite the prevalence and substantial functional, psychological, and economic impact of chronic musculoskeletal pain on military personnel and veterans, there have been few intervention studies to treat chronic pain in these populations. We conducted a randomized controlled trial to determine if a stepped- care intervention is more effective than usual care in reducing pain-related disability, pain interference, and pain severity. METHODS: We recruited patients from post-deployment and 5 general medicine clinics at a Veteran Affairs Medical Center. Participants included 242 Operation Enduring Freedom and Operation Iraqi Freedom Veterans with chronic, disabling musculoskeletal pain of the cervical or lumbar spine or extremities (shoulders, knees, and hips). The intervention involved 12 weeks of analgesic treatment and optimization according to an algorithm coupled with pain self-management strategies (Step 1) followed by 12 weeks of brief cognitive behavioral therapy (Step 2). All aspects of the intervention were delivered by nurse care managers. The primary
- utcome was pain-related disability (Roland Morris Disability Scale) at 9 months. We also assessed pain
interference (Brief Pain Inventory) and pain severity (Graded Chronic Pain Scale). The primary analysis compared the change from baseline to 9 months between study groups. To estimate treatment effects, we used random-effect linear regression adjusted for age, sex, severity of pain, and baseline value of outcome measure. Analyses were conducted with SAS version 9.13. RESULTS: There were no significant baseline differences between stepped-care intervention and usual care
- arm. The mean age of ESCAPE participants was 36.7 years (range = 21 to 73 years) and 88.4% were men. In
terms of racial mix, 77.7% were white, 13.0% were black, and 9.2% classified as other. The primary site of pain was the low back (57%) followed by knee pain (21.6%), neck pain (7.5%), shoulder pain (7.1%), and hip pain (6.6%). Two-thirds (66.4%) had been in the Army, 74.9% had been deployed to Iraq, 8.8% deployed to Afghanistan, and 16.3% deployed to both conflicts. 121 intervention participants and 120 usual care participants were included in the primary analysis. At 9 months, the mean decrease from baseline in the Roland Morris Disability Scale score was 1.6 points (95% confidence interval [CI] 0.72-2.6) in the usual care group and 3.4 points (95% CI 2.5-4.3) in the stepped-care intervention group (between group difference of -1.8 points, -3.1 to
- 0.51; p=0.0063). The mean decrease from baseline in the Brief Pain Inventory interference score was 0.86
points in the usual care group and 1.6 points in the intervention group (between group difference of -0.69 points, -1.3 to -0.12; p = 0.0170). The Graded Chronic Pain Scale severity score was reduced by 7.1% (95 CI's 2.7% to 11.5%) and 20.4% (95% CIs 14.3% to 26.6%), respectively (between group difference 13.3%, 11.6% to 15.1%; p = 0.0013). CONCLUSIONS: A stepped-care intervention that combined analgesics, self-management strategies, and brief cognitive behavioral therapy resulted in a significant reduction in pain-related disability, pain interference, and pain severity in Veterans of Iraq and Afghanistan with chronic, disabling musculoskeletal pain of the spine and extremities.
SLIDE 6 THE MEDICATION METRONOME: A HEALTH IT SYSTEM TO IMPROVE MEDICATION MANAGEMENT AND LABORATORY MONITORING FOR CHRONIC DISEASES Steven J. Atlas1; Michael Jernigan1; Jeffrey M. Ashburner1; Jaime Chang1; Leila H. Borowsky1; Yuchiao Chang1; Richard W. Grant2. 1Massachusetts General Hospital, Boston, MA; 2Kaiser Permanente Northern California, Oakland, CA. (Tracking ID #1938604) BACKGROUND: Lack of timely medication intensification and inadequate safety monitoring are two prevalent and potentially modifiable barriers to effective and safe chronic care. To test a model of chronic disease management in which medication initiation or dose adjustment orders are explicitly and immediately linked to future planned laboratory monitoring, we developed a novel health information technology (IT) tool (Medication Metronome) designed to support non-visit based medication management. Integrated into an existing electronic health record (EHR), the tool enabled primary care physicians (PCPs) to schedule future laboratory monitoring when initiating or adjusting doses of medications for diabetes, hypertension, and/or hyperlipidemia management. We hypothesized that scheduling follow-up laboratory monitoring (e.g. HbA1c 3 months after starting metformin) would support a cycle of laboratory monitoring and iterative medication dose adjustment resulting in more effective and safer chronic disease care. METHODS: Physicians from two sites within a primary care network were randomized to intervention (n=22)
- r control (n=22) groups. During a 1-year intervention, PCPs allocated to the intervention had an additional
feature in their electronic medication prescription interface that enabled them to schedule future laboratory tests when ordering new prescriptions or adjusting doses to treat type 2 diabetes, hypertension, or hyperlipidemia. This process initiated automated patient reminders that included a mailed letter and lab slip one week before the test was due and (if necessary) a second letter and lab slip one week after the test due date if no result was
- found. Notification of persistently overdue lab results (> 3 weeks after due date) was added to a physician
"Watchlist" of test results within the EHR. Control physicians had access to the same EHR but without the added Medication Metronome interface. Efficacy labs were defaulted to order, while safety monitoring needed to be actively turned on by intervention physicians. The primary effectiveness outcome was the percentage of follow-up time that a patient was at or below risk factor goal (HbA1c ≤ 7% among diabetics prescribed hypoglycemic agents; LDL-cholesterol ≤ 130 mg/dl for patients with hyperlipidemia without cardiovascular risk and ≤ 100 mg/dl for patients with cardiovascular risk) using a mixed effects model. The primary safety
- utcome was the percentage of safety monitoring laboratory tests (creatinine after initiating drugs for
hypertension and diabetes, and liver function testing after initiating statins) completed within 4 weeks of the medication order using logistic regression models. Models accounted for clustering by PCP and adjusted for patient age, gender, race/ethnicity, primary language spoken and baseline lab value. RESULTS: During the study period, there were 2991 eligible medications orders among 2031 patients of intervention PCPs and 2420 orders among 1590 patients of control PCPs. In the intervention group, 659 prescriptions (22%) used the Metronome interface to initiate laboratory follow-up (521 [79%] efficacy, 138 [21%] safety). Patient characteristics were similar among intervention and control groups except slightly more intervention patients were non-Hispanic whites (84.3% vs. 80.5%, p=0.02) and spoke English (95.4% vs. 92.8%, p=0.001), and had lower LDL levels (118.2 vs. 125.6 mg/dl, p=0.002). The adjusted percentage of time that a patient was at or below the effectiveness outcome goal over 3 months after a medication order did not differ among patients of intervention and control PCPs for diabetes (30.9% vs. 29.1%, p=0.72) or hyperlipidemia (51.6% vs. 46.7%, p=0.2) (see Table). Similarly, the performance of safety monitoring labs within 4 weeks of a medication order for hypertension, diabetes or hyperlipidemia did not differ among intervention or control groups (data not shown). CONCLUSIONS: A visit-independent, health IT tool to support a cycle of laboratory monitoring and iterative medication dose adjustment following the initiation or change of chronic disease medications during an office- based visit did not increase goal attainment or safety monitoring rates compared to usual care. New models for
SLIDE 7
reimbursing providers for health care services may be needed before adoption of innovative tools that support visit-independent medication management.