
SLIDE 1
University of California, San Francisco | Bixby Center for Global Reproductive Health
A world post Roe v. Wade
Daniel Grossman, MD
October 2019 UCSF Obstetrics and Gynecology Update
Disclosures
⇾ I have nothing to disclose
Objectives ⇾Review potential scenarios that could weaken or overturn Roe ⇾What can we expect in areas with limited
- r no access to clinic-based abortion
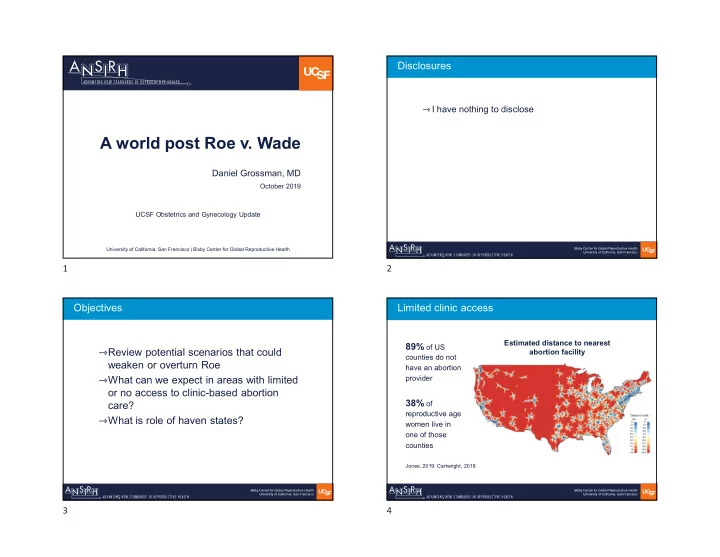
care? ⇾What is role of haven states? Limited clinic access
89% of US
counties do not have an abortion provider
38% of
reproductive age women live in
- ne of those
counties Estimated distance to nearest abortion facility
Jones, 2019; Cartwright, 2018