
SLIDE 1
5/11/2013 1
CLUBFOOT: NON-ORTHOPAEDIC SURGEON HEALTHCARE PROVIDERS ARE A VALUABLE TOOL IN TREATMENT
KATIE FREEMAN, MD ELIANA DELGADO, MD AMANDA WHITAKER, MD UNIVERSITY OF CALIFORNIA SAN FRANCISCO
58th Annual LeRoy C. Abbott Society Scientific Program May 10th, 2013
I have no disclosures
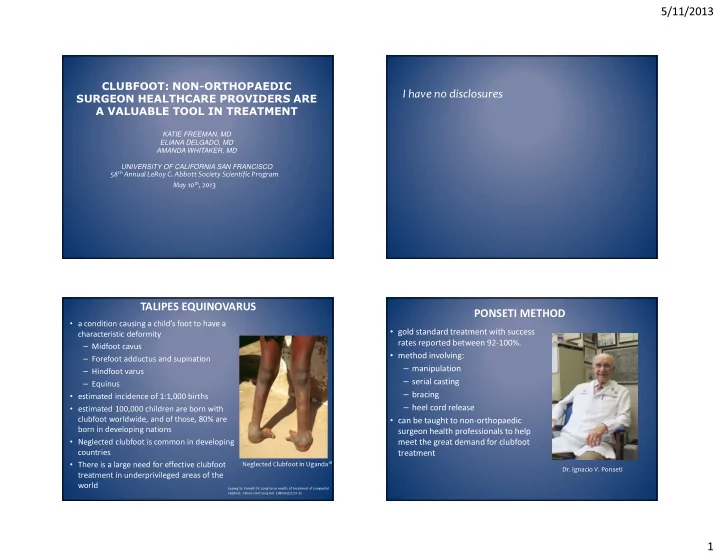
- a condition causing a child’s foot to have a
characteristic deformity – Midfoot cavus – Forefoot adductus and supination – Hindfoot varus – Equinus
- estimated incidence of 1:1,000 births
- estimated 100,000 children are born with
clubfoot worldwide, and of those, 80% are born in developing nations
- Neglected clubfoot is common in developing
countries
- There is a large need for effective clubfoot
treatment in underprivileged areas of the world
TALIPES EQUINOVARUS
Neglected Clubfoot in Uganda18
Laaveg SJ, Ponseti IV. Long-term results of treatment of congenital
- clubfoot. J Bone Joint Surg Am. 1980;62(1):23-31
- gold standard treatment with success
rates reported between 92-100%.
- method involving:
– manipulation – serial casting – bracing – heel cord release
- can be taught to non-orthopaedic
surgeon health professionals to help meet the great demand for clubfoot treatment
PONSETI METHOD
- Dr. Ignacio V. Ponseti