
SLIDE 1
12/1/17 1
PCI for STEMI in Patients with Multivessel Disease: Culprit Vessel
- r Complete Revascularization?
December 1, 2017
John S. MacGregor, M.D., Ph.D. Professor of Medicine University of California San Francisco
Outline
- Review recent studies of treatment of MVD in STEMI: PRAMI,
CvLPRIT, DANAMI-3, PRAGUE-13.
- ACC/AHA Guideline Change.
- CULPRIT-SHOCK Trial.
- ORBITA
- FAME2
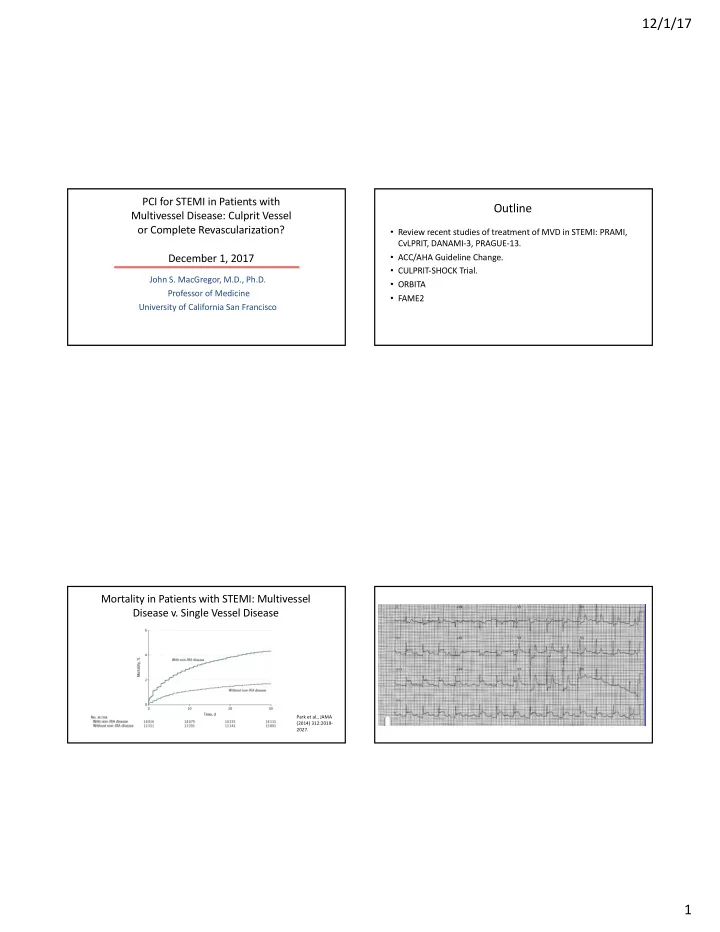
Mortality in Patients with STEMI: Multivessel Disease v. Single Vessel Disease
Park et al., JAMA (2014) 312:2019- 2027.