
1
MODULE 4 Management Strategies for Gaucher Disease Neal J. Weinreb, MD, FACP
Critical Conversations in Rare & Orphan Diseases: Challenges of Diagnosing and Caring for an Individual with Gaucher Disease
History
48 y/o woman with a 25-year history of “digestive problems” including periodic abdominal discomfort, bloating and early satiety also had chronic back and hip pain that was sometimes severe. She had easy bruising since childhood. When 38 y/o, PLT CT 72K was attributed to ITP but treatment was not needed. No other bleeding other than menorhagia. FH: “Pure” Italian. Other PH: hypothyroidism; one miscarriage.
Physical Exam
Spleen palpable 18 cm below LCM; liver 3 cm below RCM; scattered purpura arms and legs; thoracic kyphosis
Investigations
Hb 10.4 g/dL; MCV 83.3 fL; WBC 3600/µL; PLT 48,000/µL; LFTs wnl Ferritin 780ng/mL; serum iron 61 µg/dL; transferrin saturation 16% Polyclonal increase in IgG; PT, aPTT normal; Vit D 8 ng/mL L spine DEXA Z score: -2.8; Total L Femur Z score: -2.3 Abdominal ultrasound: Marked hepatosplenomegaly; cholelithiasis. MRI left and right lower extremities: Heterogeneous infiltration with medullary infarctions;
- steonecrosis and joint destruction left hip
WBC acid β-glucosidase activity: 8% of normal; consistent with GD GBA1 mutation analysis: N370S/unidentified allele
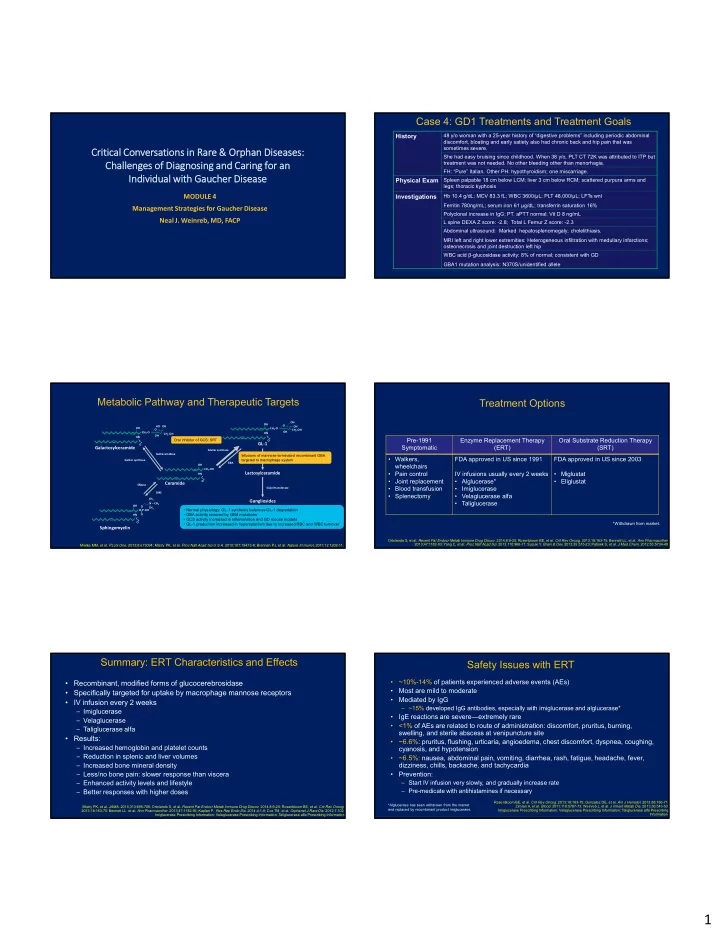
Case 4: GD1 Treatments and Treatment Goals Metabolic Pathway and Therapeutic Targets
Ceramide
OH C O CH2‐OH HN LacCer synthase Sialyl transferaseLactosylceramide Gangliosides
GluCer synthase GBA GalCer synthase GalCeramidaseGalactosylceramide
SMS SMaseSphingomyelin
OH C O O‐P‐OH HN O O = N – CH3 CH3 CH3 O OH C O CH2‐O HN HO OH OH CH2‐OHGL‐1
O OH C O CH2‐O HN OH OH CH2‐OH OH- Normal physiology: GL-1 synthesis balances GL-1 degradation
- GBA activity reduced by GBA mutations
- GCS activity increased in inflammation and GD mouse models
- GL-1 production increased in hypersplenism due to increased RBC and WBC turnover
Treatment Options
Ortolando S, et al. Recent Pat Endocr Metab Immune Drug Discov. 2014;8:9-25; Rosenbloom BE, et al. Crit Rev Oncog. 2013;18:163-75; Bennett LL, et al. Ann Pharmacother. 2013;47:1182-93; Yang C, et al. Proc Natl Acad Sci. 2013;110:966-71; Suzuki Y. Brain & Dev. 2013;35:515-23; Patnaik S, et al. J Med Chem. 2012;55:5734-48. *Withdrawn from market.Pre-1991 Symptomatic Enzyme Replacement Therapy (ERT) Oral Substrate Reduction Therapy (SRT)
- Walkers,
wheelchairs
- Pain control
- Joint replacement
- Blood transfusion
- Splenectomy
FDA approved in US since 1991 IV infusions usually every 2 weeks
- Alglucerase*
- Imiglucerase
- Velaglucerase alfa
- Taliglucerase
FDA approved in US since 2003
- Miglustat
- Eliglustat
Summary: ERT Characteristics and Effects
- Recombinant, modified forms of glucocerebrosidase
- Specifically targeted for uptake by macrophage mannose receptors
- IV infusion every 2 weeks
– Imiglucerase – Velaglucerase – Taliglucerase alfa
- Results:
– Increased hemoglobin and platelet counts – Reduction in splenic and liver volumes – Increased bone mineral density – Less/no bone pain: slower response than viscera – Enhanced activity levels and lifestyle – Better responses with higher doses
Mistry PK, et al. JAMA. 2015;313:695-706; Ortolando S, et al. Recent Pat Endocr Metab Immune Drug Discov. 2014;8:9-25; Rosenbloom BE, et al. Crit Rev Oncog. 2013;18:163-75; Bennett LL, et al. Ann Pharmacother. 2013;47:1182-93; Kaplan P. Res Rep Endo Dis. 2014;4:1-8; Cox TM, et al. Orphanet J Rare Dis. 2012;7:102; Imiglucerase Prescribing Information; Velaglucerase Prescribing Information; Taliglucerase alfa Prescribing InformationSafety Issues with ERT
- ~10%-14% of patients experienced adverse events (AEs)
- Most are mild to moderate
- Mediated by IgG
– ~15% developed IgG antibodies, especially with imiglucerase and alglucerase*
- IgE reactions are severe—extremely rare
- <1% of AEs are related to route of administration: discomfort, pruritus, burning,
swelling, and sterile abscess at venipuncture site
- ~6.6%: pruritus, flushing, urticaria, angioedema, chest discomfort, dyspnea, coughing,
cyanosis, and hypotension
- ~6.5%: nausea, abdominal pain, vomiting, diarrhea, rash, fatigue, headache, fever,
dizziness, chills, backache, and tachycardia
- Prevention:
– Start IV infusion very slowly, and gradually increase rate – Pre-medicate with antihistamines if necessary
Rosenbloom BE, et al. Crit Rev Oncog. 2013;18:163-75; Gonzalez DE, et al. Am J Hematol. 2013;88:166-71; Zimran A, et al. Blood. 2011;118:5767-73; Weinreb J, et al. J Inherit Metab Dis. 2013;36:543-53; Imiglucerase Prescribing Information; Velaglucerase Prescribing Information; Taliglucerase alfa Prescribing Information. *Alglucerase has been withdrawn from the market and replaced by recombinant product imiglucerase.