
SLIDE 1
1
Impact of Sensitivity and Specificity on Sample Size for Biomarker Trial Design
Lucinda Billingham
Professor of Biostatistics Director, MRC Midland Hub for Trials Methodology Research Biostatistics Lead, Cancer Research UK Clinical Trials Unit University of Birmingham Joint Meeting of RSS Medical Section and MHTMR University of Birmingham, June 30th 2010
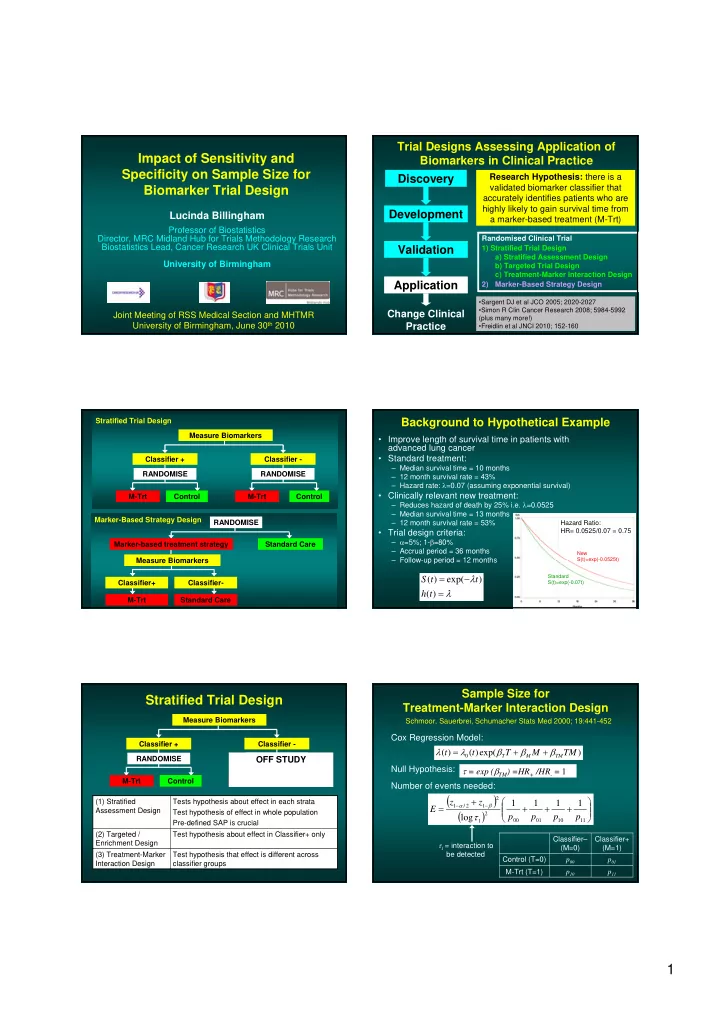
Trial Designs Assessing Application of Biomarkers in Clinical Practice Discovery Development Validation Application
Change Clinical Practice
Randomised Clinical Trial 1) Stratified Trial Design a) Stratified Assessment Design b) Targeted Trial Design c) Treatment-Marker Interaction Design 2) Marker-Based Strategy Design
- Sargent DJ et al JCO 2005; 2020-2027
- Simon R Clin Cancer Research 2008; 5984-5992
(plus many more!)
- Freidlin et al JNCI 2010; 152-160
Research Hypothesis: there is a validated biomarker classifier that accurately identifies patients who are highly likely to gain survival time from a marker-based treatment (M-Trt)
Measure Biomarkers Classifier + Classifier - RANDOMISE M-Trt Control Control M-Trt RANDOMISE Stratified Trial Design Marker-Based Strategy Design RANDOMISE Marker-based treatment strategy Standard Care Classifier+ Classifier- Standard Care Measure Biomarkers M-Trt
Background to Hypothetical Example
- Improve length of survival time in patients with
advanced lung cancer
- Standard treatment:
– Median survival time = 10 months – 12 month survival rate = 43% – Hazard rate: =0.07 (assuming exponential survival)
- Clinically relevant new treatment:
– Reduces hazard of death by 25% i.e. =0.0525 – Median survival time = 13 months – 12 month survival rate = 53%
- Trial design criteria:
– =5%; 1-=80% – Accrual period = 36 months – Follow-up period = 12 months
) ( ) exp( ) ( t h t t S
New S(t)=exp(-0.0525t) Standard S(t)=exp(-0.07t)
Hazard Ratio: HR= 0.0525/0.07 = 0.75
Measure Biomarkers Classifier + Classifier - RANDOMISE M-Trt Control Control M-Trt RANDOMISE
OFF STUDY
Stratified Trial Design
Test hypothesis that effect is different across classifier groups (3) Treatment-Marker Interaction Design Test hypothesis about effect in Classifier+ only Tests hypothesis about effect in each strata Test hypothesis of effect in whole population Pre-defined SAP is crucial (2) Targeted / Enrichment Design (1) Stratified Assessment Design
Sample Size for Treatment-Marker Interaction Design
p11 p10 M-Trt (T=1) p01 p00 Control (T=0) Classifier+ (M=1) Classifier– (M=0)
11 10 01 00 2 1 2 1 2 / 1
1 1 1 1 log p p p p z z E
1 = interaction to be detected Schmoor, Sauerbrei, Schumacher Stats Med 2000; 19:441-452
) exp( ) ( ) ( TM M T t t
TM M T