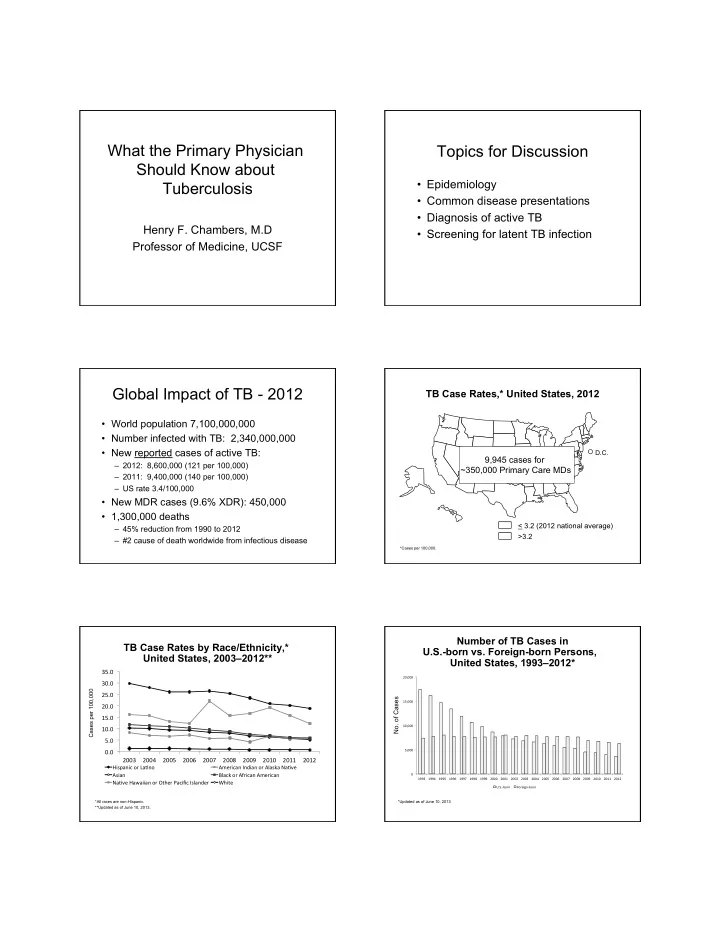

What the Primary Physician Should Know about Tuberculosis
Henry F. Chambers, M.D Professor of Medicine, UCSF
Topics for Discussion
- Epidemiology
- Common disease presentations
- Diagnosis of active TB
- Screening for latent TB infection
Global Impact of TB - 2012
- World population 7,100,000,000
- Number infected with TB: 2,340,000,000
- New reported cases of active TB:
– 2012: 8,600,000 (121 per 100,000) – 2011: 9,400,000 (140 per 100,000) – US rate 3.4/100,000
- New MDR cases (9.6% XDR): 450,000
- 1,300,000 deaths
– 45% reduction from 1990 to 2012 – #2 cause of death worldwide from infectious disease
TB Case Rates,* United States, 2012
*Cases per 100,000.
< 3.2 (2012 national average) >3.2
D.C.
9,945 cases for ~350,000 Primary Care MDs
TB Case Rates by Race/Ethnicity,* United States, 2003–2012**
*All races are non-Hispanic. **Updated as of June 10, 2013.
Cases per 100,000
0.0 ¡ 5.0 ¡ 10.0 ¡ 15.0 ¡ 20.0 ¡ 25.0 ¡ 30.0 ¡ 35.0 ¡ 2003 ¡ 2004 ¡ 2005 ¡ 2006 ¡ 2007 ¡ 2008 ¡ 2009 ¡ 2010 ¡ 2011 ¡ 2012 ¡
Hispanic ¡or ¡La7no ¡ American ¡Indian ¡or ¡Alaska ¡Na7ve ¡ Asian ¡ Black ¡or ¡African ¡American ¡ Na7ve ¡Hawaiian ¡or ¡Other ¡Pacific ¡Islander ¡ White ¡
Number of TB Cases in U.S.-born vs. Foreign-born Persons, United States, 1993–2012*
*Updated as of June 10, 2013
- No. of Cases
0 ¡ 5,000 ¡ 10,000 ¡ 15,000 ¡ 20,000 ¡ 1993 ¡ 1994 ¡ 1995 ¡ 1996 ¡ 1997 ¡ 1998 ¡ 1999 ¡ 2000 ¡ 2001 ¡ 2002 ¡ 2003 ¡ 2004 ¡ 2005 ¡ 2006 ¡ 2007 ¡ 2008 ¡ 2009 ¡ 2010 ¡ 2011 ¡ 2012 ¡ U.S.-‑born ¡ Foreign-‑born ¡