
SLIDE 1
4/15/2016 1
Thoracic Central Venous Obstruction (T-CVO) A New Look at an Old Problem
Bart Dolmatch, MD, FSIR
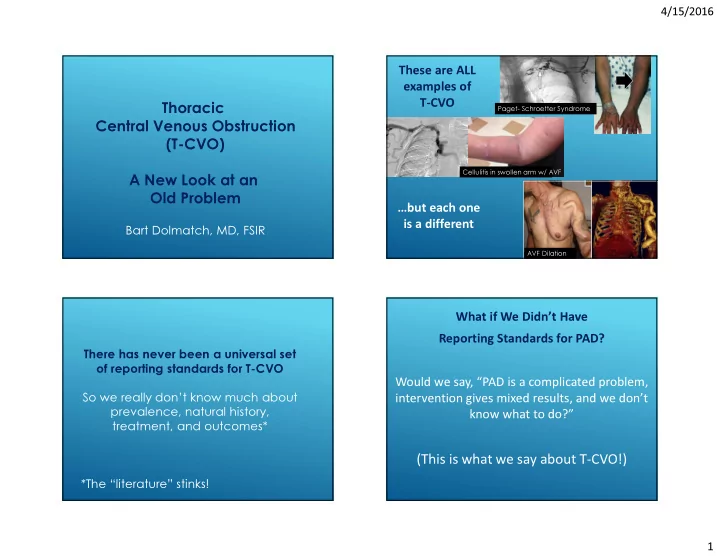
Cellulitis in swollen arm w/ AVF Paget- Schroetter Syndrome
These are ALL examples of T-CVO …but each one is a different
AVF Dilation
There has never been a universal set
- f reporting standards for T-CVO