
SLIDE 1
4/21/2018 1
Surgical Approach to Treatment
- f Pulmonary Vein Stenosis
Christopher Caldarone, MD 11th International Conference on Neonatal and Childhood Pulmonary Vascular Disease San Francisco 2018 04 21
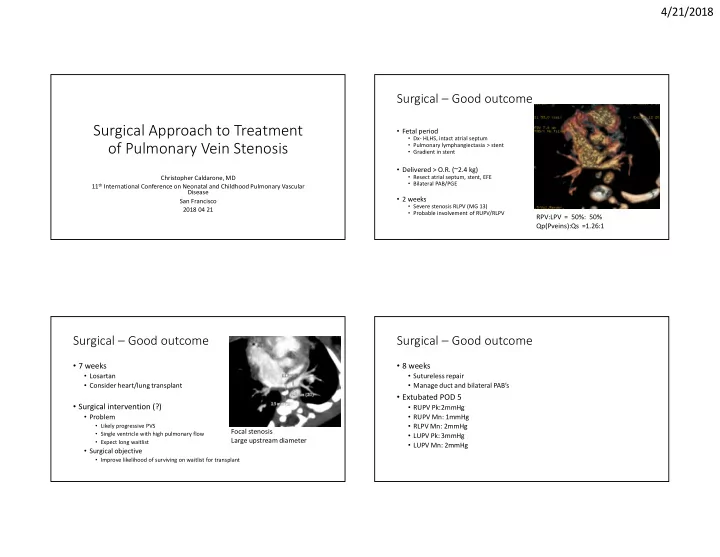
Surgical – Good outcome
- Fetal period
- Dx- HLHS, intact atrial septum
- Pulmonary lymphangiectasia > stent
- Gradient in stent
- Delivered > O.R. (~2.4 kg)
- Resect atrial septum, stent, EFE
- Bilateral PAB/PGE
- 2 weeks
- Severe stenosis RLPV (MG 13)
- Probable involvement of RUPV/RLPV
RPV:LPV = 50%: 50% Qp(Pveins):Qs =1.26:1
Surgical – Good outcome
- 7 weeks
- Losartan
- Consider heart/lung transplant
- Surgical intervention (?)
- Problem
- Likely progressive PVS
- Single ventricle with high pulmonary flow
- Expect long waitlist
- Surgical objective
- Improve likelihood of surviving on waitlist for transplant
Focal stenosis Large upstream diameter
Surgical – Good outcome
- 8 weeks
- Sutureless repair
- Manage duct and bilateral PAB’s
- Extubated POD 5
- RUPV Pk:2mmHg
- RUPV Mn: 1mmHg
- RLPV Mn: 2mmHg
- LUPV Pk: 3mmHg
- LUPV Mn: 2mmHg