
SLIDE 1
1 | [footer text here]
Zuckerberg San Francisco General
HIV for the Primary Care Provider
Elizabeth Imbert, MD MPH Division of HIV, ID and Global Medicine
Zuckerberg San Francisco General
- I have no disclosures.
Zuckerberg San Francisco General
Roadmap
- HIV epidemiology
- HIV prevention
- HIV testing & disclosure
- Antiretroviral treatment
considerations
- OIs and OI prophylaxis
Key Messages:
- Test all
- Treat all
- Treat early
- caution with some
OIs
- ART: Simple, tolerable
combinations preferred
- Goal is viral suppression
Zuckerberg San Francisco General
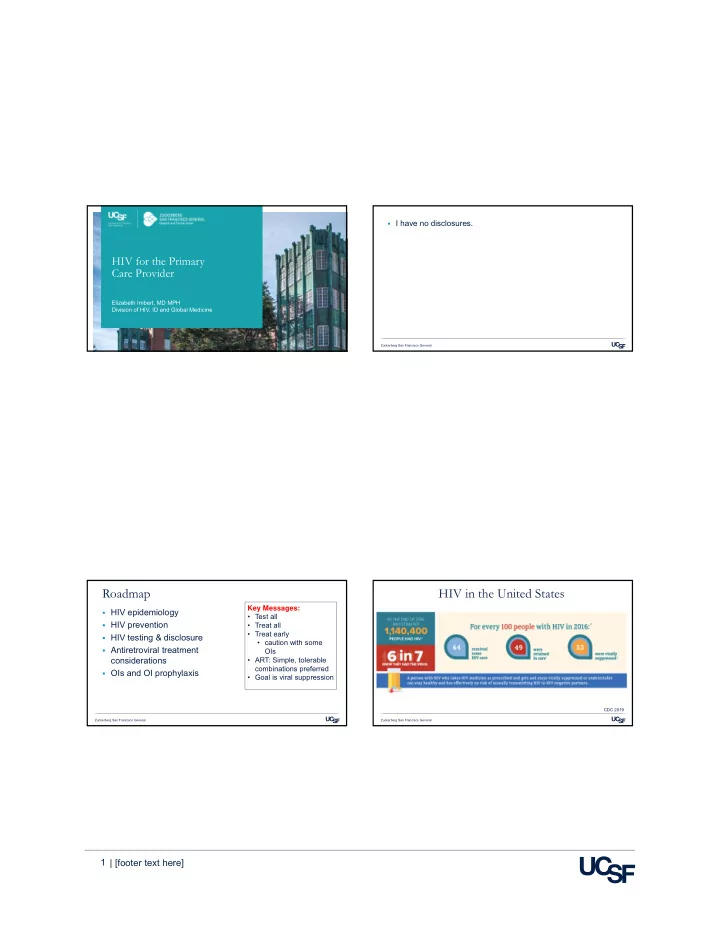
HIV in the United States
CDC 2019