
SLIDE 1
12/1/17 1
Liviu Klein MD, MS
Associate Professor Director, Mechanical Circulatory Support and Heart Failure Device Programs Liviu.Klein@ucsf.edu
Reducing Readmissions in Heart Failure
2
Financial Relationship Disclosure
I will NOT discuss off label/ investigational use of products. The following financial relationships exist: Consultant: Abbott, Boston Scientific, Medtronic.
Reducing Readmissions in Heart Failure
3
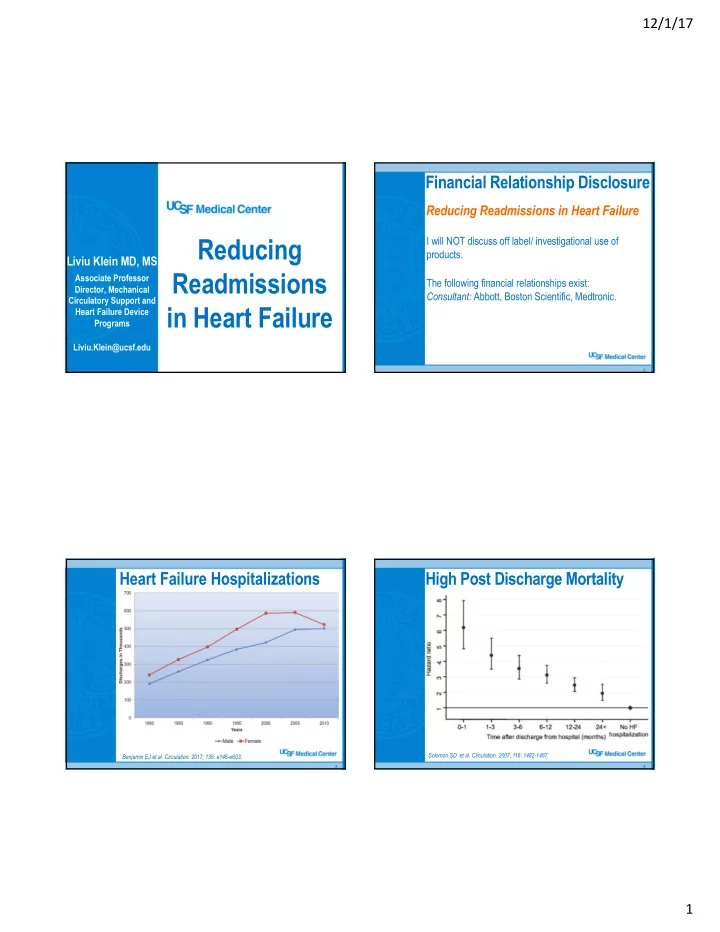
Heart Failure Hospitalizations
Benjamin EJ et al. Circulation. 2017; 135: e146-e603.
4
High Post Discharge Mortality
Solomon SD et al. Circulation. 2007; 116: 1482-1487.