
SLIDE 1
12/15/2018 1
Recognition and Management of Inflammatory Back Pain: Essentials for Primary Care Providers
Lianne S. Gensler, MD
University of California, San Francisco
Disclosures
- Advisor/consultant: Galapagos, Janssen, Lilly
- Research grant/support: Amgen, Novartis, Pfizer, UCB
Case
- A 27-year-old woman with low back pain that started 2 years
- ago. She experienced initially alternating “hip” pain, worse in
the morning, with stiffness lasting 45 minutes. The pain is made better with exercise and NSAIDs.
- Pain awakens her from sleep around 4 AM and requires
getting up to take ibuprofen and stretch.
NSAIDs = nonsteroidal anti-inflammatory drugs.
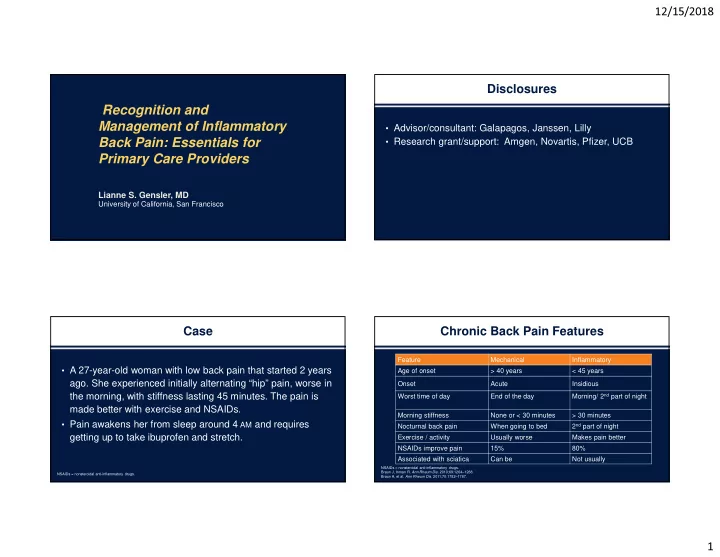
Chronic Back Pain Features
NSAIDs = nonsteroidal anti-inflammatory drugs. Braun J, Inman R. Ann Rheum Dis. 2010;69:1264–1268. Braun A, et al. Ann Rheum Dis. 2011;70:1782–1787.