
SLIDE 1
1
Prostate Cancer 2016
Smarter Screening and Risk-Adapted Treatment
Matthew R. Cooperberg, MD, MPH Departments of Urology and Epidemiology & Biostatistics 44th Annual Advances in Internal Medicine May 25, 2016 @dr_coops
Departm ent of Urology
T
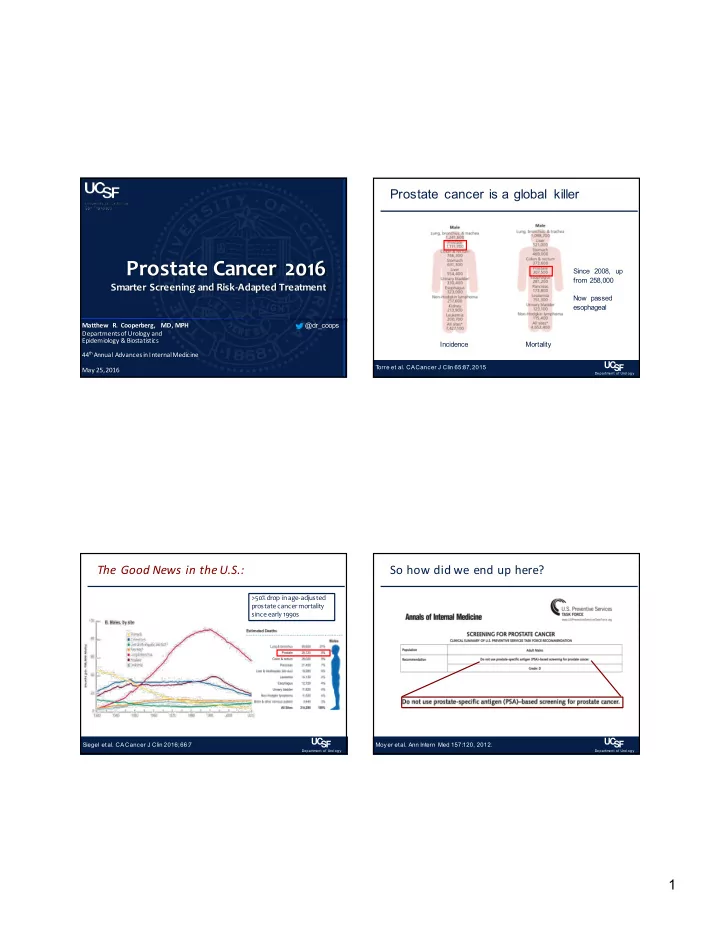
- rre et al. CA Cancer J Clin 65:87, 2015
Prostate cancer is a global killer
Incidence Mortality Since 2008, up from 258,000 Now passed esophageal
Departm ent of Urology
Siegel et al. CA Cancer J Clin 2016; 66:7
The Good News in the U.S.:
>50% drop in age-adjusted prostate cancer mortality since early 1990s
Departm ent of Urology
Moyer et al. Ann Intern Med 157:120, 2012.