
SLIDE 1
1
12/13/2018
Carlin Senter, MD Associate Professor UCSF Primary Care Sports Medicine
Image Challenge: Hip, Foot and Ankle
UCSF Primary Care Sports Medicine Conference 2018 Anthony Luke, MD, MPH Professor
Name the 3 hip ROM tests the in order in which they are performed here:
The 3 hip ROM tests in order are:
- A. Extension, flexion, adduction
- B. Extension, flexion, abduction
- C. Flexion, abduction, adduction
- D. Flexion, adduction, abduction
- E. Flexion, external rotation, internal rotation
- F. Flexion, internal rotation, external rotation
E x t e n s i
- n
, f l e x i
- n
, a d d u c . . . E x t e n s i
- n
, f l e x i
- n
, a b d u c . . . F l e x i
- n
, a b d u c t i
- n
, a d d u . . . F l e x i
- n
, a d d u c t i
- n
, a b d u . . . F l e x i
- n
, e x t e r n a l r
- t
a t i
- n
, . . . F l e x i
- n
, i n t e r n a l r
- t
a t i
- n
, . . .
1% 0% 19% 71% 3% 6%
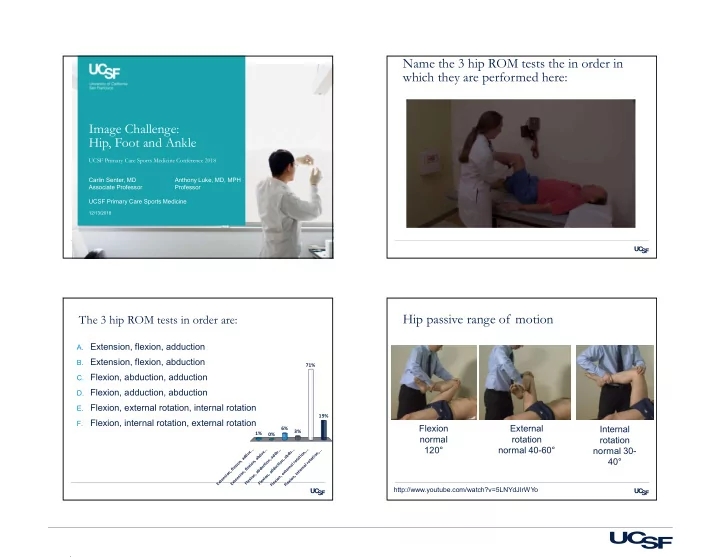
Hip passive range of motion
Flexion normal 120° External rotation normal 40-60° Internal rotation normal 30- 40°
http://www.youtube.com/watch?v=5LNYdJIrWYo