
SLIDE 1
6/12/16 1
Medical Futility:
When is Enough Enough?
Robert D. Truog, MD
Professor of Medical Ethics, Anaesthesiology & Pediatrics Harvard Medical School Senior Associate in Critical Care Medicine Boston Children’s Hospital
Disclosure
I have no actual or potential conflict of interest in relation to this program/ presentation.
I’m afraid there’s very little I can do
I’m afraid there’s really very little I can do…
Baby Janvier
- Janvier was a 2 year old who had been born
with a large frontal encephalocoele
- Janvier’s parents were young, homeless
- Janvier was never responsive and never showed
any signs of neurologic development
- He was an inpatient almost continually for two
years, with frequent electrolyte abnormalities related to diabetes insipidus
Baby Janvier
- Staff consistently communicated
recommendation for comfort care
- Intensive involvement of ethics consultation
service and psychosocial support services
- Parents never agreed to any limitations of care
- At two years of age, he was found cyanotic on
the ward, and was rushed to the ICU
- The question: should we perform CPR?
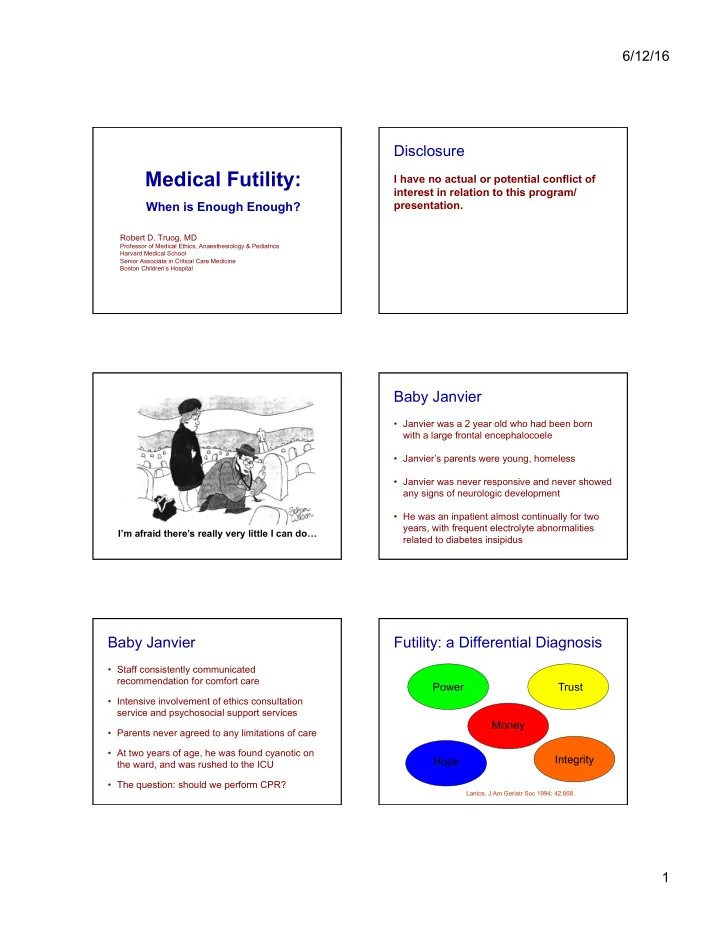
Futility: a Differential Diagnosis
- Lantos. J Am Geriatr Soc 1994; 42:868.