
SLIDE 1
Maine’s State Innovation Model (SIM) Grant
Presented to the Maine Medical Association by Commissioner Mary C. Mayhew July 24, 2013
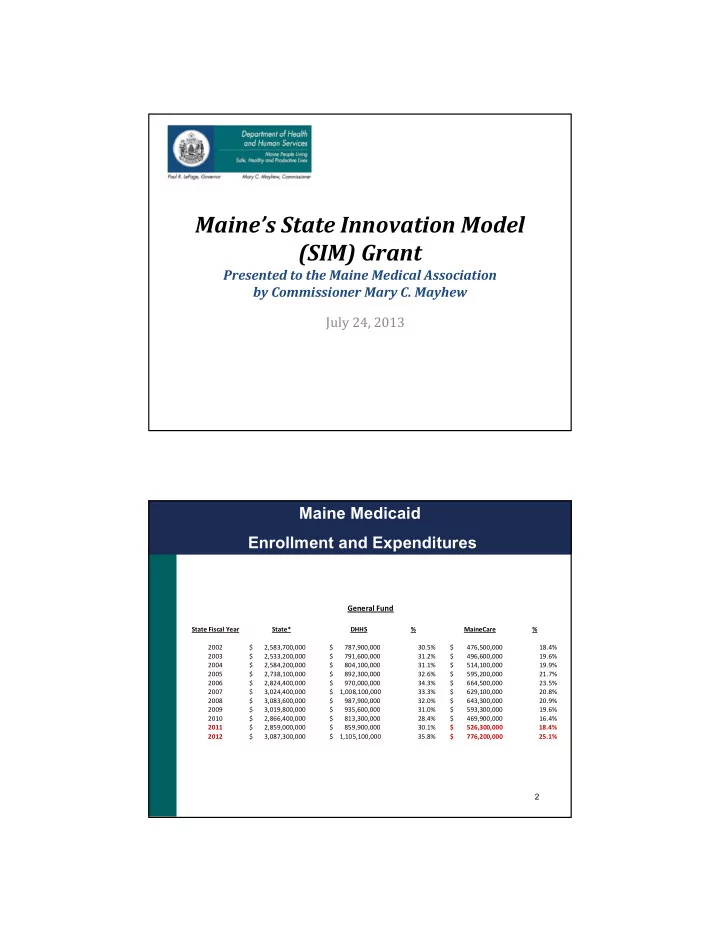
Maine Medicaid Enrollment and Expenditures
2 General Fund
State Fiscal Year State* DHHS % MaineCare % 2002 $ 2,583,700,000 $ 787,900,000 30.5% $ 476,500,000 18.4% 2003 $ 2,533,200,000 $ 791,600,000 31.2% $ 496,600,000 19.6% 2004 $ 2,584,200,000 $ 804,100,000 31.1% $ 514,100,000 19.9% 2005 $ 2,738,100,000 $ 892,300,000 32.6% $ 595,200,000 21.7% 2006 $ 2,824,400,000 $ 970,000,000 34.3% $ 664,500,000 23.5% 2007 $ 3,024,400,000 $ 1,008,100,000 33.3% $ 629,100,000 20.8% 2008 $ 3,083,600,000 $ 987,900,000 32.0% $ 643,300,000 20.9% 2009 $ 3,019,800,000 $ 935,600,000 31.0% $ 593,300,000 19.6% 2010 $ 2,866,400,000 $ 813,300,000 28.4% $ 469,900,000 16.4% 2011 $ 2,859,000,000 $ 859,900,000 30.1% $ 526,300,000 18.4% 2012 $ 3,087,300,000 $ 1,105,100,000 35.8% $ 776,200,000 25.1%