
SLIDE 1
Journal of Rawalpindi Medical College (JRMC); 2017;21(3): 308-310 308 Case Report
Infected Polycystic Liver Disease- An Unusual Presentation
- f Extra-renal Autosomal Dominant Polycystic Kidney
Disease (ADPKD)
Mohammad Hourani and Daniyal Nagi
Department of Internal Medicine, Tawam Hospital, Al-Ain, UAE
Introduction
Autosomal dominant polycystic kidney disease (ADPKD) is characterized by the progressive expansion of multiple bilateral renal cysts leading to enlargement and distortion of the kidney and ultimately, end-stage renal disease . ADPKD is the most common inherited cause of kidney disease associated with both PKD1 and non-PKD1 genotypes, can occur as extra-renal manifestation such as Adult Polycystic Liver Disease (APLD) or distinct disease in absence
- f
renal cysts. Typically these are asymptomatic but may be associated with infection or haemorrhage, liver function is typically preserved . 1-3
Case Report
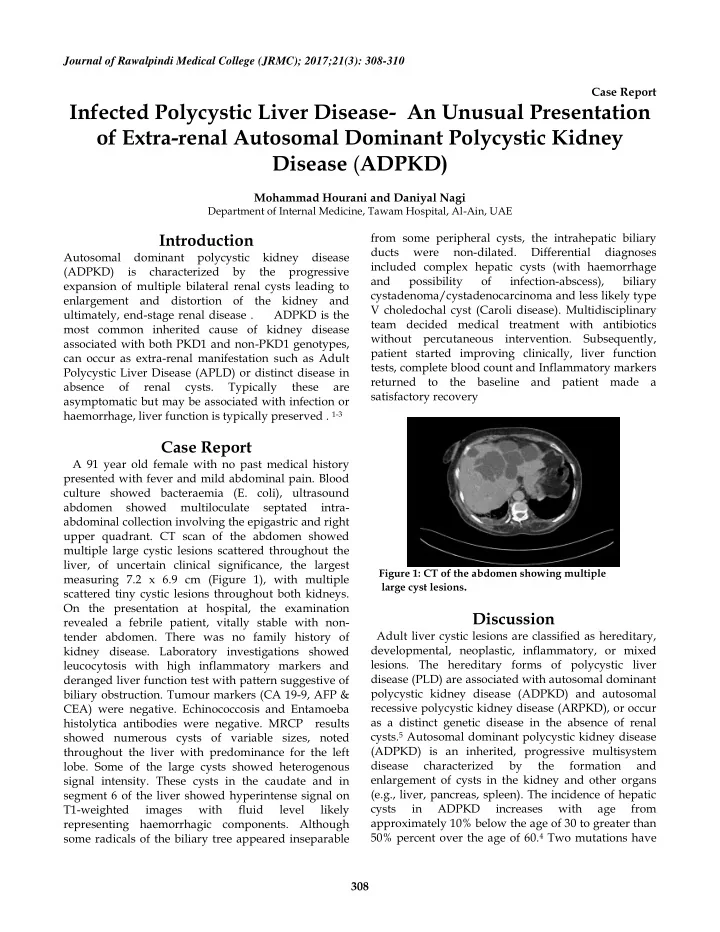
A 91 year old female with no past medical history presented with fever and mild abdominal pain. Blood culture showed bacteraemia (E. coli), ultrasound abdomen showed multiloculate septated intra- abdominal collection involving the epigastric and right upper quadrant. CT scan of the abdomen showed multiple large cystic lesions scattered throughout the liver, of uncertain clinical significance, the largest measuring 7.2 x 6.9 cm (Figure 1), with multiple scattered tiny cystic lesions throughout both kidneys. On the presentation at hospital, the examination revealed a febrile patient, vitally stable with non- tender abdomen. There was no family history of kidney disease. Laboratory investigations showed leucocytosis with high inflammatory markers and deranged liver function test with pattern suggestive of biliary obstruction. Tumour markers (CA 19-9, AFP & CEA) were negative. Echinococcosis and Entamoeba histolytica antibodies were negative. MRCP results showed numerous cysts of variable sizes, noted throughout the liver with predominance for the left
- lobe. Some of the large cysts showed heterogenous
signal intensity. These cysts in the caudate and in segment 6 of the liver showed hyperintense signal on T1-weighted images with fluid level likely representing haemorrhagic components. Although some radicals of the biliary tree appeared inseparable from some peripheral cysts, the intrahepatic biliary ducts were non-dilated. Differential diagnoses included complex hepatic cysts (with haemorrhage and possibility
- f
infection-abscess), biliary cystadenoma/cystadenocarcinoma and less likely type V choledochal cyst (Caroli disease). Multidisciplinary team decided medical treatment with antibiotics without percutaneous intervention. Subsequently, patient started improving clinically, liver function tests, complete blood count and Inflammatory markers returned to the baseline and patient made a satisfactory recovery
Figure 1: CT of the abdomen showing multiple large cyst lesions.
Discussion
Adult liver cystic lesions are classified as hereditary, developmental, neoplastic, inflammatory, or mixed
- lesions. The hereditary forms of polycystic liver