
1
Hyperlipidemia
Vasudevan A. Raghavan MBBS,MD,MRCP(UK)
Assistant Professor, Department of Internal Medicine, Ohio State University Medical Center, Divisions of Endocrinology, Diabetes and Metabolism and Cardiovascular Sciences Clinical Lipidologist, The Ross Heart Hospital Comprehensive Lipid Management Clinic
Be it known ….!
- “It should be noted that these guidelines
are intended to inform, not replace, the physician’s clinical judgment, which must ultimately determine the appropriate treatment for each individual.”
Ref: Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III
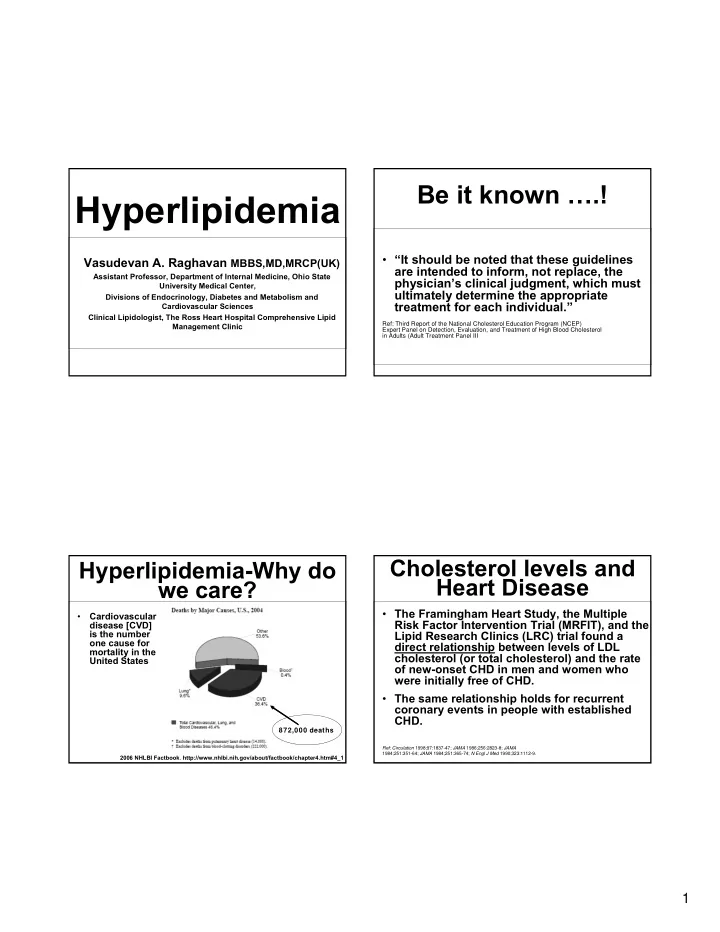
Hyperlipidemia-Why do we care?
- Cardiovascular
disease [CVD] is the number
- ne cause for
mortality in the United States
2006 NHLBI Factbook. http://www.nhlbi.nih.gov/about/factbook/chapter4.htm#4_1
872,000 deaths
Cholesterol levels and Heart Disease
- The Framingham Heart Study, the Multiple
Risk Factor Intervention Trial (MRFIT), and the Lipid Research Clinics (LRC) trial found a direct relationship between levels of LDL cholesterol (or total cholesterol) and the rate
- f new-onset CHD in men and women who
were initially free of CHD.
- The same relationship holds for recurrent
coronary events in people with established CHD.
Ref: Circulation 1998;97:1837-47; JAMA 1986;256:2823-8; JAMA 1984;251:351-64; JAMA 1984;251:365-74; N Engl J Med 1990;323:1112-9.