
SLIDE 1
6/27/2019 1
Laboratory Management in a Crisis: Experiences with Ebola
Vicki Herrera, MS – Research Coordinator University of Nebraska Medical Center, Nebraska Public Health Laboratory
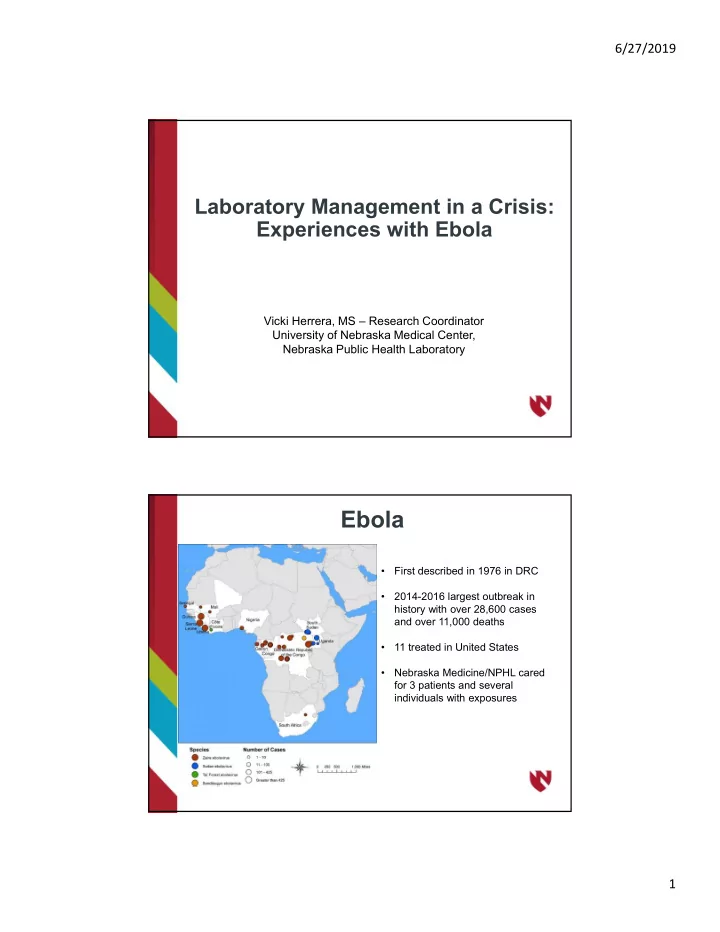
Ebola
- First described in 1976 in DRC
- 2014-2016 largest outbreak in
history with over 28,600 cases and over 11,000 deaths
- 11 treated in United States
- Nebraska Medicine/NPHL cared
for 3 patients and several individuals with exposures