SLIDE 4 5/24/2018 4
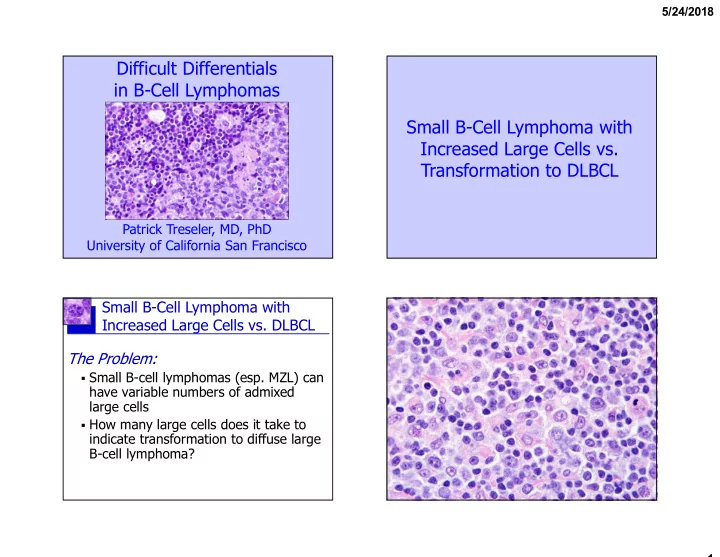
Small B-Cell Lymphoma with Increased Large Cells vs. DLBCL The Solution (for MALT lymphoma at least):
- Solid clusters (dozens to hundreds?)
- r diffuse sheets of large cells
- Make sure you are not looking at a
B-cell follicle (use a CD21 stain)!
- If large cells are increased but fall
short of clear-cut DLBCL, be descriptive & share your concern
“The presence of diffuse areas composed entirely or predominantly of large centroblasts (that would fulfil the criteria for grade 3 FL) in FL of any grade is equivalent to DLBCL, and a separate diagnosis of DLBCL should be made.”
Transformation of Follicular Lymphoma to DLBCL
ES Jaffe et al. Follicular lymphoma. In: WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues (Swerdlow et al., eds). Lyon, France: International Agency for Research on Cancer, 2017, pp. 266-73.
Definition according to 2017 WHO…
- Meets criteria for grade 3 FL
- Architecture entirely diffuse (CD21)
Follicular Lymphoma
ES Jaffe et al. Follicular lymphoma. In: WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues (Swerdlow et al., eds). Lyon, France: International Agency for Research on Cancer, 2017, pp. 266-73.
Grading per 2017 WHO
Grade* Definition
Grade 1-2 (low grade) 0-15 centroblasts/HPF 1 0-5 centroblasts/HPF 2 6-15 centroblasts/HPF Grade 3 (high grade) >15 centroblasts/HPF 3A Centrocytes present 3B Solid sheets of centroblasts
*WHO grading method derived from method of Mann and Berard (Mann RB, Berard CW. Criteria for the cytologic subclassification of follicular lymphomas: a proposed alternative method. Hematol Oncol. 1983 Apr-Jun;1(2):187-92.)
Grading of Follicular Lymphoma
Practically all centrocytes; centroblasts present, but a little hard to find.
Cos Berard’s actual “eyeball” method (per Nancy Harris)
Centroblasts easy to find, but mainly single scattered cells, and clearly in the minority
Lots of centroblasts, often forming clusters