
SLIDE 1
12/9/2016 1
Top Shoulder Problems in Primary Care: raise your hand if you want to know more
Christina Allen, M.D.
Clinical Professor UCSF Sports Medicine Disclosures
- OREF (Orthopaedic Research and
Education Foundation) - Research Grant Recipient
- Major Duke Fan
2
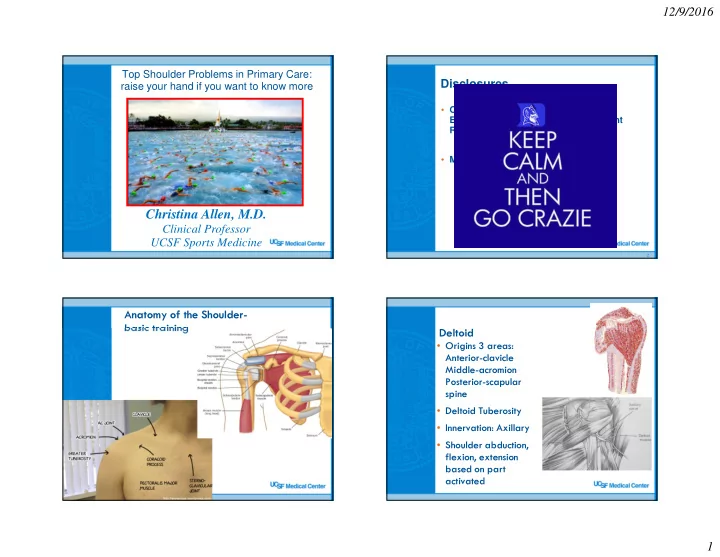
Anatomy of the Shoulder- basic training Deltoid
- Origins 3 areas:
Anterior-clavicle Middle-acromion Posterior-scapular spine
- Deltoid Tuberosity
- Innervation: Axillary
- Shoulder abduction,