
SLIDE 1
1
Medicine Boards Certification Review
Infectious Diseases, Part 2
Lisa G. Winston, MD University of California, San Francisco Division of HIV, ID, and Global Medicine and Division of Hospital Medicine Zuckerberg San Francisco General Hospital and Trauma Center
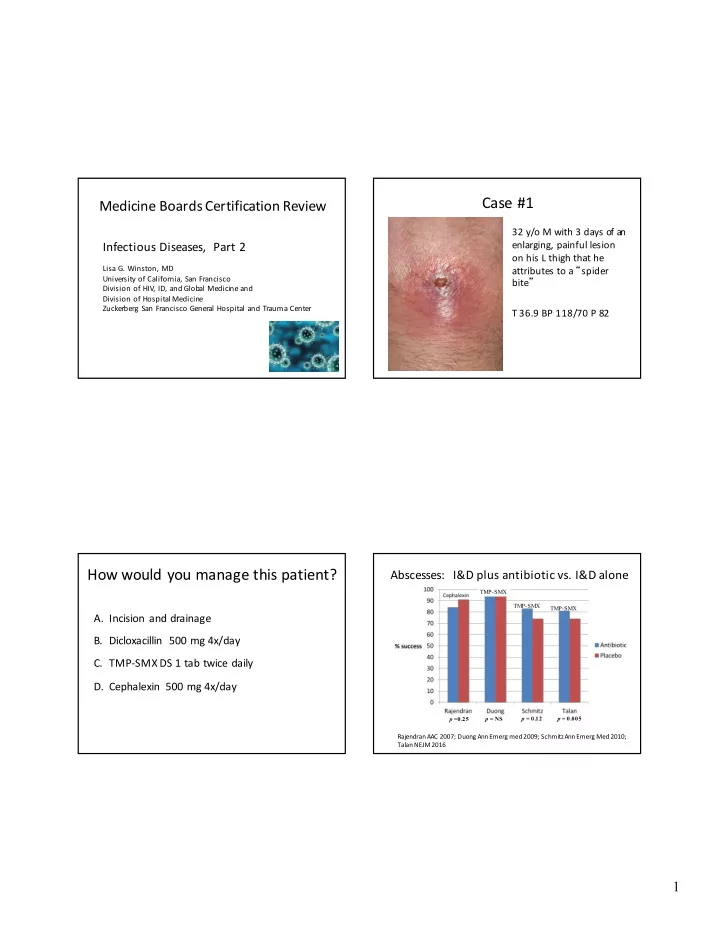
Case #1
32 y/o M with 3 days of an enlarging, painful lesion
- n his L thigh that he
attributes to a “spider bite” T 36.9 BP 118/70 P 82
How would you manage this patient?
- A. Incision and drainage
- B. Dicloxacillin 500 mg 4x/day
- C. TMP-SMX DS 1 tab twice daily
- D. Cephalexin 500 mg 4x/day
Abscesses: I&D plus antibiotic vs. I&D alone
TMP-SMX TMP-SMX TMP-SMX p =0.25 p = NS p = 0.12 p = 0.005
RajendranAAC 2007; Duong Ann Emerg med 2009; Schmitz Ann Emerg Med 2010; Talan NEJM 2016