
SLIDE 1
3/2/2018 1
Neeta Thakur MD MPH Neeta.Thakur@ucsf.edu
Care of Underserved Patient with COPD 03/01/2018 Disclosures
- Neeta Thakur, MD MPH
- Spouse is employee at Roche/Genentech
Learning Objectives
- To review the burden of COPD
- To review the updates in COPD guidelines using a case-base approach
- Screening
- Categorizing
- Treatment
- To learn the evidence for and options for implementing adjunct therapies for patients with COPD from
vulnerable populations
- Education
- Exercise
- Emerging Threats COPD and Climate Change
- Hot Days
- Trigger exposure
- Air Pollution
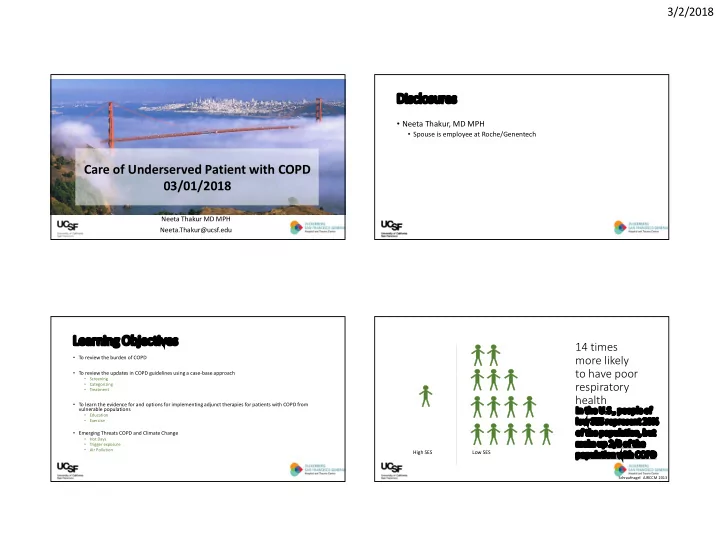
14 times more likely to have poor respiratory health
High SES Low SES
Schraufnagel AJRCCM 2013
In the U.S., people of low SES represent 20%
- f the population, but
make up 2/3 of the population with COPD