
Solving Clinical Challenges in
Bipolar Disorder
Terence A. Ketter, MD
Professor Emeritus Department of Psychiatry and Behavioral Sciences Stanford University School of Medicine Stanford, California
Overview
Bipolar Disorder – Solving Clinical Challenges
Ketter TA (Ed). Advances in Treatment of Bipolar Disorders. Arlington, VA: American Psychiatric Publishing, Inc.; 2015.
- 1. Diagnostic Nosology
– Challenges distinguishing bipolar from unipolar
- 2. Pharmacologic Treatment
– Challenges with therapeutic vs side effects
- 3. Adverse Events
– Challenges with weight gain/sedation and akathisia 4. Non-Pharmacologic Treatment – Challenges with access to evidence-based Rx
- I. Diagnostic Nosology
Challenges with Accurate Diagnosis
Diagnostic Boundaries of Bipolar Disorder
ADHD = attention-deficit/hyperactivity disorder; CD = conduct disorder; MDD = major depressive disorder; ODD =
- ppositional defiant disorder.
Ketter TA (Ed). Advances in Treatment of Bipolar Disorders. Arlington, VA: American Psychiatric Publishing, Inc.; 2015.
- Complex, variable phenomenology
– Different subtypes, mood states, courses, age-dependent presentations
- Crucial differential diagnosis
– MDD
- Confounding comorbidities
– Substance abuse, anxiety disorders – Disruptive behavioral (ADHD, ODD, CD), cluster B disorders
- Measures to enhance diagnostic accuracy
– Collateral information – DSM Screening
- Mood Disorders Questionnaire
– Beyond DSM
- Onset age, atypical symptoms, course, treatment effects,
family history
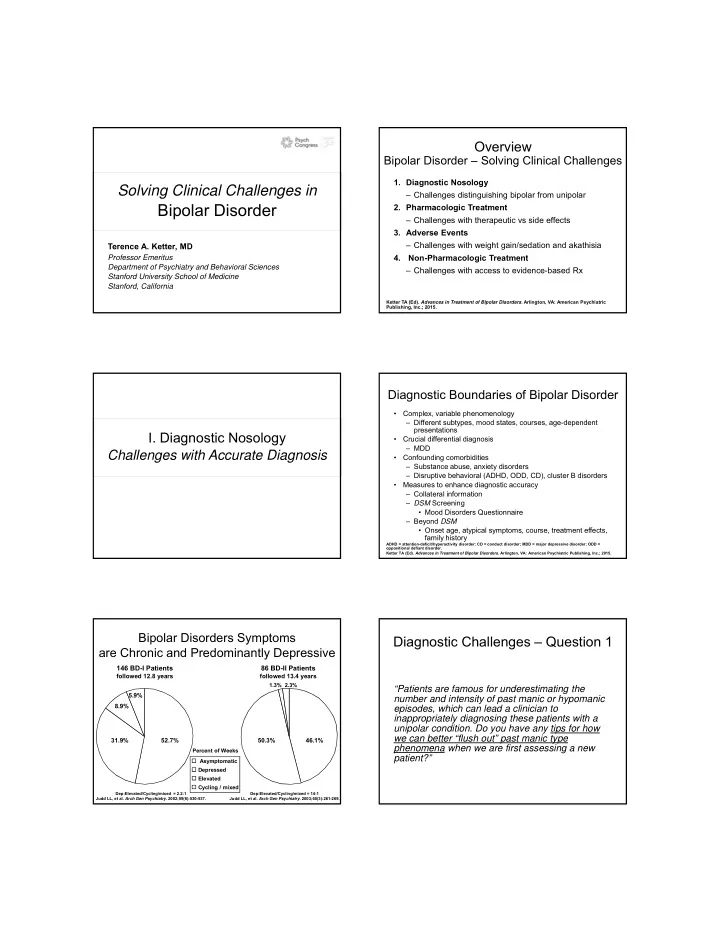
Bipolar Disorders Symptoms are Chronic and Predominantly Depressive
52.7% 31.9% 8.9% 5.9%
Asymptomatic Depressed Elevated Cycling / mixed Percent of Weeks
146 BD-I Patients
followed 12.8 years
86 BD-II Patients
followed 13.4 years 46.1% 50.3%
1.3% 2.3%
Dep:Elevated/Cycling/mixed = 14:1 Judd LL, et al. Arch Gen Psychiatry. 2003;60(3):261-269. Dep:Elevated/Cycling/mixed = 2.2:1 Judd LL, et al. Arch Gen Psychiatry. 2002;59(6):530-537.