
SLIDE 1
5/24/2018 1
Kirk D. Jones, MD UCSF Dept of Pathology kirk.jones@ucsf.edu
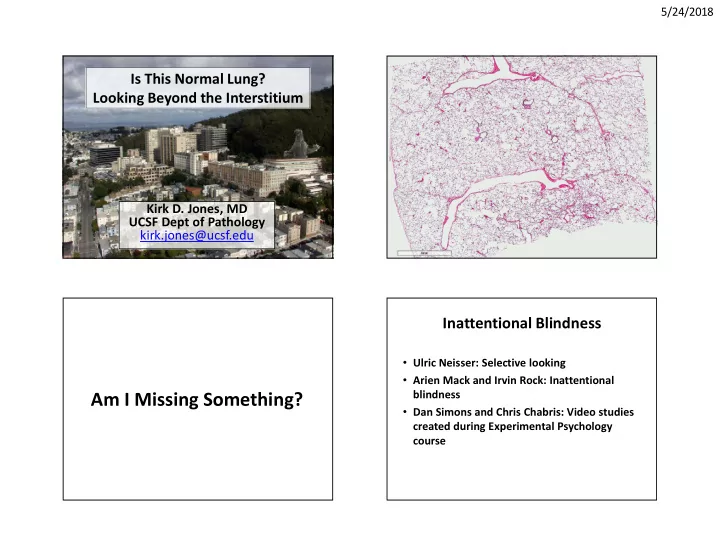
Is This Normal Lung? Looking Beyond the Interstitium
Am I Missing Something?
Inattentional Blindness
- Ulric Neisser: Selective looking
- Arien Mack and Irvin Rock: Inattentional
blindness
- Dan Simons and Chris Chabris: Video studies