
SLIDE 1
8/8/2013 1
Substance Use Disorders in Primary Care: Screening, Brief Interventions, Pharmacotherapy
Katherine Julian, M.D.
UCSF Division of General Internal Medicine August 7, 2013
A Real Case…
31 yo man presenting to resident clinic for new
patient appt
Recently hospitalized with new onset atrial
- fibrillation. Resolved with cardioversion. Given
coumadin and presenting to titrate this medication.
Prompted to take an alcohol history→binge
drinking with indications of alcohol dependence
Quiz…Your Clinic Panel
In your clinic panel, what percentage of your current clinic patients would be classified with alcohol abuse or dependence*?
<1% 2-5% 6-9% 10% 20%
0% 14% 27% 35% 24%
- A. <1%
- B. 2-5%
- C. 6-9%
- D. 10%
- E. 20%
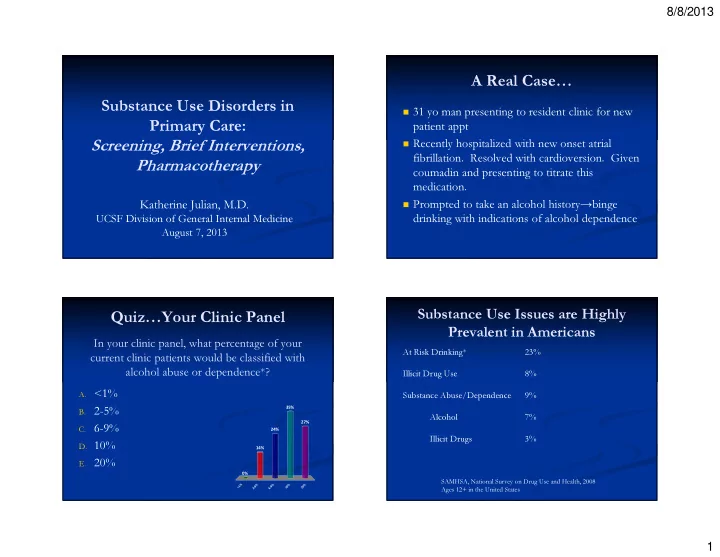
Substance Use Issues are Highly Prevalent in Americans
At Risk Drinking* 23% Illicit Drug Use 8% Substance Abuse/Dependence 9% Alcohol 7% Illicit Drugs 3%
SAMHSA, National Survey on Drug Use and Health, 2008 Ages 12+ in the United States