
Alyssa Buono, MD-R, Kelli Davis, DO-R, Erin Ricker, MD
A Code Curriculum at Your Fingertips: Improving Performance and Resident Confidence in Pediatric Codes A Code Curriculum at Your Fingertips: Improving Performance and Resident Confidence in Pediatric Codes
Prisma Health – University of South Carolina School of Medicine
- 1. Anderson, L. W., Berg, K. M., Saindon, B. Z., Massaro, J. M., et al. (2015). Time to Epinephrine
and Survival After Pediatric In-Hospital Cardiac Arrest. Journal of American Medical Association, 314(8), 802-810.
- 2. Hunt, E. A., Duval-Arnould, J.M., Bembea, M.M., et al. (2018). Association Between Time to
Defibrillation and Survival in Pediatric In-Hospital Cardiac Arrest With a First Documented Shockable
- Rhythm. Journal of American Medical Association Network Open, 1(5):e182643.
- 3. Hunt, E. A., Jeffers, J., McNamara, L., Newton, H., et al. (2018). Improved Cardiopulmonary
Resuscitation Performance With CODE ACES: A Resuscitation Quality Bundle. Journal of American Heart Association.
- 4. Hunt, E. A., Walker, A. R., Shaffner, D. H., Miller, M.R., Pronovost, P. J. (2008). Simulation of In-
Hospital Pediatric Medical Emergencies and Cardiopulmonary Arrests: Highlighting the Importance
- f the First 5 Minutes. Pediatrics, 121(1), e34-e43.
- 5. Nadel, F.M., Lavelle, J.M, Fein, J.A., et al. (2000). Assessing Pediatric Senior Residents’ Training
in Resuscitation: Fund of Knowledge, Technical Skills, and Perception of Confidence. Pediatric Emergency Care, 16(2):73-76.
- 6. Pediatric Mock Code Toolkit. (2012). Retrieved from
https://www.luriechildrens.org/globalassets/documents/emsc/education/mockcode2nded20122.pdf.
- 7. Sam, J., Pierse, M., Al-Qahtani, A., et al. (2012). Implementation and Evaluation of a Simulation
Curriculum for Pediatric Residency Programs Including Just-In-Time In Situ Mock Codes. Paediatrics & Child Health, 17(2): e16-e20.
- 8. Tibbals, J. and Kinney, S. (2006). A Prospective Study of Outcome of In-Patient Paediatric
Cardiopulmonary Arrest. Resuscitation, 71(3), 310-318.
Introduction
- The incidence of pediatric cardiopulmonary arrests is low but the majority of pediatric
codes tend to have poor outcomes, with an average survival-to-discharge rate of 14- 36% 1,3,8
- Data suggests that a shorter time to epinephrine, initiation of chest compressions
and prompt defibrillation are critical to improve outcomes in pediatric codes 1,2
- Studies have demonstrated deficiencies in pediatric residents’ confidence and
knowledge in managing codes, and have identified a need for routine multidisciplinary mock codes 4,5,6,7
- Barriers include fear, anxiety, low exposure, and poor long term retention and
translation of annual PALS training to real or mock resuscitation 5,6
- At Prisma Health Children’s Hospital, a resident code curriculum was first initiated in
July 2018 which was shown to increase pediatric residents’ self-confidence and code quiz scores but no significant improvement in mock code times
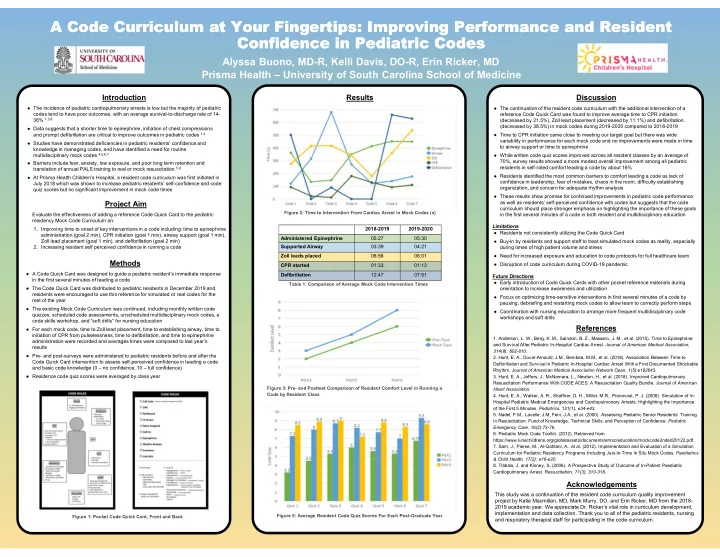
Results Discussion
- The continuation of the resident code curriculum with the additional intervention of a
reference Code Quick Card was found to improve average time to CPR initiation (decreased by 21.5%), Zoll lead placement (decreased by 11.1%) and defibrillation. (decreased by 38.5%) in mock codes during 2019-2020 compared to 2018-2019
- Time to CPR initiation came close to meeting our target goal but there was wide
variability in performance for each mock code and no improvements were made in time to airway support or time to epinephrine
- While written code quiz scores improved across all resident classes by an average of
70%, survey results showed a more modest overall improvement among all pediatric residents in self-rated comfort leading a code by about 16%
- Residents identified the most common barriers to comfort leading a code as lack of
confidence in leadership, fear of mistakes, chaos in the room, difficulty establishing
- rganization, and concern for adequate rhythm analysis
- These results show promise for continued improvements in pediatric code performance
as well as residents’ self-perceived confidence with codes but suggests that the code curriculum should place stronger emphasis on highlighting the importance of these goals in the first several minutes of a code in both resident and multidisciplinary education Limitations
- Residents not consistently utilizing the Code Quick Card
- Buy-in by residents and support staff to treat simulated mock codes as reality, especially
during times of high patient volume and stress
- Need for increased exposure and education to code protocols for full healthcare team
- Disruption of code curriculum during COVID-19 pandemic
Future Directions
- Early introduction of Code Quick Cards with other pocket reference materials during
- rientation to increase awareness and utilization
- Focus on optimizing time-sensitive interventions in first several minutes of a code by
pausing, debriefing and restarting mock codes to allow team to correctly perform steps
- Coordination with nursing education to arrange more frequent multidisciplinary code
workshops and soft drills
Methods
- A Code Quick Card was designed to guide a pediatric resident’s immediate response
in the first several minutes of leading a code
- The Code Quick Card was distributed to pediatric residents in December 2019 and
residents were encouraged to use this reference for simulated or real codes for the rest of the year
- The existing Mock Code Curriculum was continued, including monthly written code
quizzes, scheduled code assessments, unscheduled multidisciplinary mock codes, a code skills workshop, and “soft drills” for nursing education
- For each mock code, time to Zoll lead placement, time to establishing airway, time to
initiation of CPR from pulselessness, time to defibrillation, and time to epinephrine administration were recorded and averages times were compared to last year’s results
- Pre- and post-surveys were administered to pediatric residents before and after the
Code Quick Card intervention to assess self-perceived confidence in leading a code and basic code knowledge (0 – no confidence, 10 – full confidence)
- Residence code quiz scores were averaged by class year
References Project Aim
Evaluate the effectiveness of adding a reference Code Quick Card to the pediatric residency Mock Code Curriculum on:
- 1. Improving time to onset of key interventions in a code including: time to epinephrine
administration (goal 2 min), CPR initiation (goal 1 min), airway support (goal 1 min), Zoll lead placement (goal 1 min), and defibrillation (goal 2 min)
- 2. Increasing resident self perceived confidence in running a code
Acknowledgements
This study was a continuation of the resident code curriculum quality improvement project by Katie Macmillan, MD, Mark Murry, DO, and Erin Ricker, MD from the 2018- 2019 academic year. We appreciate Dr. Ricker’s vital role in curriculum development, implementation and data collection. Thank you to all of the pediatric residents, nursing and respiratory therapist staff for participating in the code curriculum.
Figure 1: Pocket Code Quick Card, Front and Back Figure 3: Pre- and Posttest Comparison of Resident Comfort Level in Running a Code by Resident Class Figure 5: Average Resident Code Quiz Scores For Each Post-Graduate Year 2018-2019 2019-2020 Administered Epinephrine 05:27 05:30 Supported Airway 03:39 04:21 Zoll leads placed 06:56 06:01 CPR started 01:33 01:13 Defibrillation 12:47 07:51 Table 1: Comparison of Average Mock Code Intervention Times Figure 2: Time to Intervention From Cardiac Arrest in Mock Codes (s)