
Cheap Shots: Update on Vaccinations
David J. Quan, Pharm.D., BCPS Pharmacist Specialist-Solid Organ Transplant UCSF Health Health Sciences Clinical Professor of Pharmacy UCSF School of Pharmacy
2Goal and Objectives
Goal:
- Provide the clinician with an overview of some recent
developments in vaccinations relevant to transplantation. Objectives:
- Discuss the mechanism and function of vaccines
- Review some recently FDA approved vaccines:
- Hepatitis B Vaccine recombinant, adjuvanted (Heplisav-B)
- Meningococcal Group B Vaccine (Bexsero & Trumenba)
- Zoster vaccine recombinant, adjuvanted (Shingrix)
- Review some useful vaccination resources available
“
3“An ounce of prevention is worth a pound of cure.”
- Benjamin Franklin
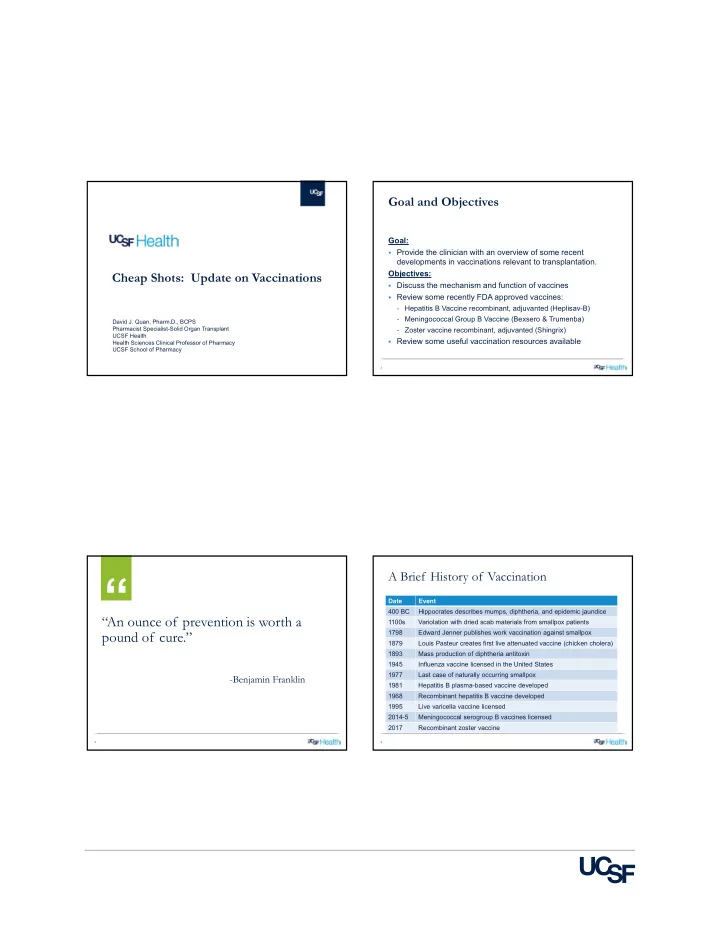
A Brief History of Vaccination
Date Event 400 BC Hippocrates describes mumps, diphtheria, and epidemic jaundice 1100s Variolation with dried scab materials from smallpox patients 1798 Edward Jenner publishes work vaccination against smallpox 1879 Louis Pasteur creates first live attenuated vaccine (chicken cholera) 1893 Mass production of diphtheria antitoxin 1945 Influenza vaccine licensed in the United States 1977 Last case of naturally occurring smallpox 1981 Hepatitis B plasma-based vaccine developed 1968 Recombinant hepatitis B vaccine developed 1995 Live varicella vaccine licensed 2014-5 Meningococcal serogroup B vaccines licensed 2017 Recombinant zoster vaccine