
4/12/2013 1
Presented By: Aaron Saul, Jr RN IV Access/PICC Coordinator Peterson Regional Medical Center Active member of: CENTEXVAN, AVA, INS
1492: Blood infused from 3 children into the Pope. All 3 children and the Pope died.
1638: William Harvey described the function of the Human Circulatory System.
1658: Christopher Wren used a quill and Pig’s bladder to infuse wine and opium into dogs.
1667: Successful transfusions between animals.
1818: First successful transfusion in child suffering from hemorrhage.
1832: First use of intravenous saline used to treat Cholera victims
1933: First IV solution produced.
1935: Abbott laboratories produces IV solutions for mass use in hospitals.
1940: First fulltime IV nurse in Massachusetts General.
1940 to 1946: IV skills taught to field medics in attempt to save more wounded soldiers on the battle
- field. (It should be noted that up to this point, inserting an IV was deemed to be the job of the
physician and outside the scope of nursing practice). Survival rate of wounded soldiers increased by approximately 55%.
1960: Central Venous cannulation first described.
1965: First use of PICC lines
1970-1980: More and more responsibility for IV care passed on to nurses. Development of the first dedicated IV Teams.
1990: It is documented that almost 90% of hospitalized patients receive some sort of IV therapy.
In one study, out of 30 million hospitalized Americans treated with IV medications, 5 million of those patients received their therapy through some sort of CVC.
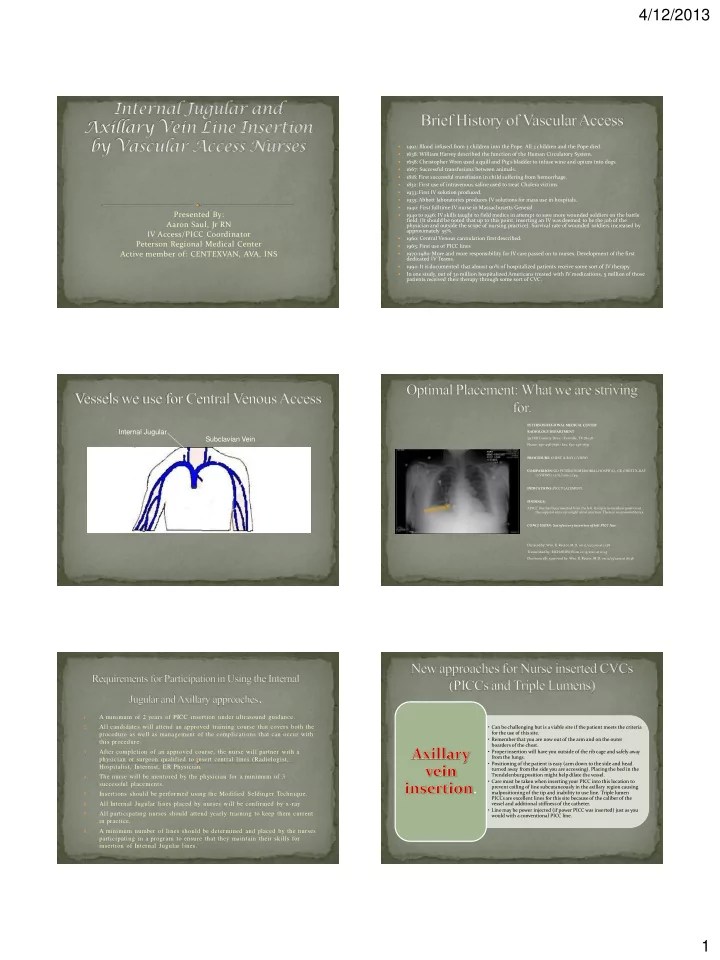
Internal Jugular External Jugular Subclavian Vein Axillary Vein Cephalic Vein Basilic Vein Brachial Vein
PETERSON REGIONAL MEDICAL CENTER RADIOLOGY DEPARTMENT 551 Hill Country Drive • Kerrville, TX 78028 Phone: 830-258-7636 • Fax: 830-258-7657 PROCEDURE: CHEST X-RAY (1 VIEW) COMPARISON: SID PETERSON MEMORIAL HOSPITAL, CR, CHEST X-RAY (2 VIEWS), 12/12/2010, 11:49. INDICATIONS: PICC PLACEMENT FINDINGS: A PICC line has been inserted from the left. Its tip is in excellent position at the superior vena cava/right atrial junction. There is no pneumothorax. CONCLUSION: Satisfactory insertion of left PICC line. Dictated by: Wm. R. Rector, M.D. on 12/13/2010 at 11:58 Transcribed by: RICHARDSON on 12/13/2010 at 12:43 Electronically approved by: Wm. R. Rector, M.D. on 12/13/2010 at 16:36
1.
A minimum of 2 years of PICC insertion under ultrasound guidance.
2.
All candidates will attend an approved training course that covers both the procedure as well as management of the complications that can occur with this procedure.
3.
After completion of an approved course, the nurse will partner with a physician or surgeon qualified to insert central lines (Radiologist, Hospitalist, Internist, ER Physician.
4.
The nurse will be mentored by the physician for a minimum of 3 successful placements.
5.
Insertions should be performed using the Modified Seldinger Technique.
6.
All Internal Jugular lines placed by nurses will be confirmed by x-ray.
7.
All participating nurses should attend yearly training to keep them current in practice.
8.
A minimum number of lines should be determined and placed by the nurses participating in a program to ensure that they maintain their skills for insertion of Internal Jugular lines.
- Can be challenging but is a viable site if the patient meets the criteria
for the use of this site.
- Remember that you are now out of the arm and on the outer
boarders of the chest.
- Proper insertion will have you outside of the rib cage and safely away
from the lungs.
- Positioning of the patient is easy (arm down to the side and head
turned away from the side you are accessing). Placing the bed in the Trendelenburg position might help dilate the vessel.
- Care must be taken when inserting your PICC into this location to
prevent coiling of line subcutaneously in the axillary region causing malpositioning of the tip and inability to use line. Triple lumen PICCs are excellent lines for this site because of the caliber of the vessel and additional stiffness of the catheter.
- Line may be power injected (if power PICC was inserted) just as you
would with a conventional PICC line.