
SLIDE 1
18-04-16 1 Fistula failure – how to use risk scores and algorithms
Charmaine Lok, MD Professor of Medicine, University of Toronto UCSF Vascular Symposium 2018 April 19, 2018 San Francisco
The BEST Hemodialysis Vascular Access A functioning FISTULA!
Fistula is 35 years old, 1 intervention no complications
Problem: Fistula Failure
- “Suitability Failure” or “Failure to Mature”
- Early thrombosis
- Failure of vessel dilatation and maturation (stenosis, collaterols)
- Difficulties with cannulation: infiltration injury
Would we recommend a fistula is these patients?
- Multiple previously failed fistula?
- Deemed “marginal” by the surgeon
- Multiple comorbidities
- Elder age e.g. >75?
- Limited life expectancy
- O’Hare, A, et al., Kidney Int, 2007
- pts >85 yrs would have 5:1 unneccessary
to necessary procedures
- Richardson, et.al, J Vasc Access, 2009
- Pts >70 yrs →50% 18 mo survival
- Fistula survival: 39% at 12 mos
- Only 35% accessed their fistulas
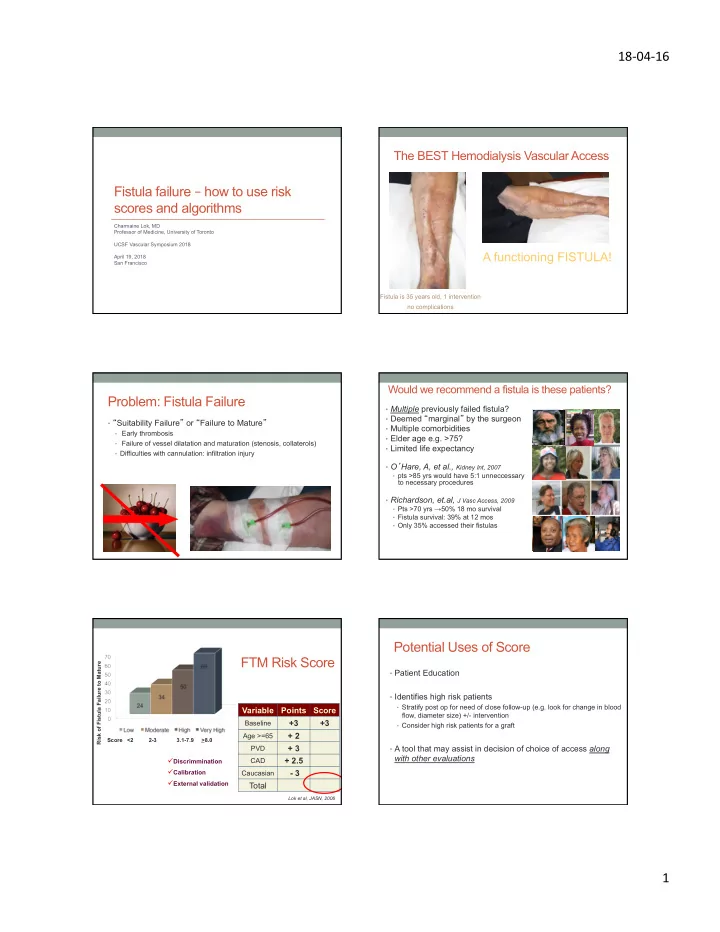
FTM Risk Score
Variable Points Score
Baseline
+3 +3
Age >=65
+ 2
PVD
+ 3
CAD
+ 2.5
Caucasian
- 3
Total
Score <2 2-3 3.1-7.9 >8.0
Lok et al, JASN, 2006
ü
Discrimmination
ü
Calibration
ü
External validation
Risk of Fistula Failure to Mature
Potential Uses of Score
- Patient Education
- Identifies high risk patients
- Stratify post op for need of close follow-up (e.g. look for change in blood
flow, diameter size) +/- intervention
- Consider high risk patients for a graft
- A tool that may assist in decision of choice of access along
with other evaluations