
SLIDE 1
3/10/2017 1
Surgical Interventions for Pulmonary Vein Stenosis
Christopher Caldarone Hospital for Sick Children, Toronto
10th International Conference Neonatal & Childhood Pulmonary Vascular Disease March 10, 2016 San Francisco
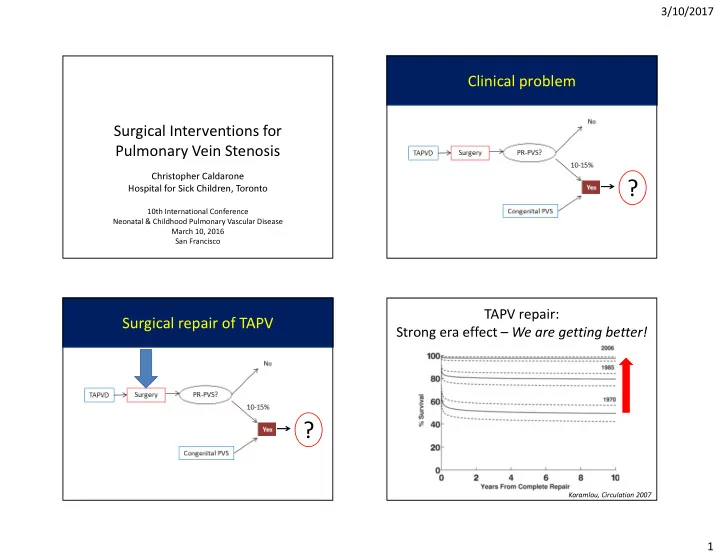
Clinical problem
?
Surgical repair of TAPV
?
TAPV repair: Strong era effect – We are getting better!
Karamlou, Circulation 2007