SLIDE 2 2
Inhibitors: Tolcapone, Pyrogallol Parkinson’s D with l-Dopa (rarely used, liver failure)
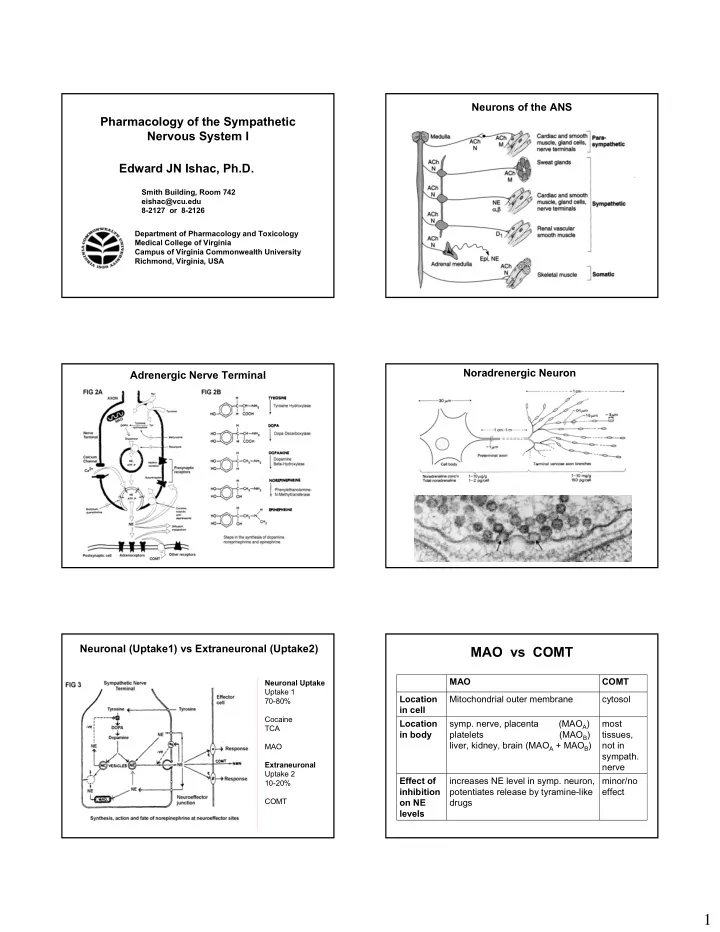
COMT MAO
Inhibitors: Non-selective Depression Tranylcypromine, Pargyline Inhibitors: Selective Depression MAO-A Clorgiline Parkinson’ D MAO-B Selegiline
MAO vs COMT
R HO HO COMT R HO CH
3O R CH2 N H R MAO R C O H R C O OH R CH2OH
Metabolism of Catecholamines
Major Metabolites VMA MOPEG Metabolism by either MAO or COMT, inactivates drug
Receptor Subtypes
α-Receptors
α2-Receptors α1-Receptors β-Receptors α1A α1B α1C α1D α2A α2B α2C α2D β1 β2 β3 1948 90’s 60’s 70’s 90’s PLC ↑Ca++ ↑IP3 DAG A/C ↑cAMP A/C ↓cAMP
RECEPTOR TISSUE ACTIONS Alpha1 most vascular smooth muscle contraction EPI > or = NE >> ISO pupillary dilator muscle contraction (dilation) pilomotor smooth muscle erects hair vas deferens contraction liver glycogenolysis intestinal smooth muscle relaxation intestinal sphincters contraction Alpha2 some vascular smooth muscle contraction NE > EPI >> ISO nerve terminals (NE & Ach) inhibit transmitter release platelets aggregation fat cells inhibition of lipolysis Beta1 heart ↑ force, rate, conduction velocity ISO > EPI = NE coronary blood vessels dilatation kidney renin release Beta2 bronchial smooth muscle relaxation ISO > or = EPI >> NE uterine smooth muscle relaxation intestinal smooth muscle relaxation vascular smooth muscle relaxation liver glycogenolysis NA nerve terminals facilitation of release Beta3 fat cells lipolysis ISO = NE > EPI
Adrenergic Agents – Relative Selectivity
↓cAMP Gs Brain, cardiovascular D2 D3 D4 ↑cAMP Gs Renal, vascular SM, brain D1, D5 ↑cAMP Gs Adipose cells β3 ↑cAMP Gs Smooth muscle, lung β2 ↑cAMP Gs Cardiac muscle, juxtaglomerular apparatus β1 ↓cAMP Gi Nerve endings, smooth smooth muscle α2 ↑Ca2+, ↑IP3, DAG Gq Effector tissues: smooth muscle, glands α1
2nd Messenger G Protein Location Receptor
Second Messengers
X
Phospholipase C
G-Protein coupled receptors Adrenergic Alpha1-receptors Cholinergic M1 M3 M5