
1
Importance of Water Quality in Dialysis and need for Endotoxin Testing
Dibyendu Maji & Soma Chatterjee / Lonza / February, 2011
slide 2
The function of kidney is to remove excess salts & waste products from the human body. Nonfunctional kidneys leads to problem in maintaining the level of sodium, potassium, and minerals and which results in congenital kidney disease.
There are two types of dialysis treatment available:
- 1. Hemodialysis
- 2. Peritoneal dialysis.
The working principle of these two methods varies slightly, but both operate
- n the same principles of replacing kidney function by eliminating the toxic
products from the blood.
The dialysis fluid consists of up to 99% of reverse osmosis water; in addition, chemicals are added, such as acids, salts and bicarbonate.
- slide 3
Indian Scenario : End Stage Kidney Disease
150,000 new patients develop end stage kidney failure each year in India Only 3 percent patients receive kidney transplant About 15-20 percent treated with dialysis 820 plus Nephrologists 710 dialysis centers 3000 dialysis machines
SK Agarwal, Chronic Kidney Disease in India: Challenges and Solutions ... Nephron Clin Pract 2009;
slide 4
Hemodialysis Treatment:
- Artificial kidney (hemodialyzer) used to remove the excretory products and fluids from
blood.
- Dialysis patient undergoes small surgery that creates an access point in an arm or leg,
and then the blood is allowed to flow through a hemodialyzer.
- Hemodialysis treatment occurs 3 times a week , each session of 4 hr duration. Each
exposure of 150 litres, one year exposure of 23400 litres of dialysis fluid.
- Actual frequency and time of Hemodialysis treatment depends upon the condition of
kidney, function, accumulation of toxic products in the blood etc. Peritoneal Dialysis treatment:
- Dialysis is done without removing the blood from the body.
- Catheter is placed in the abdomen by a minor surgery and catheter point is closed with
a solution called the dialysate, which then fills the inner side of the abdomen.
- Toxic substances in the blood filter through the blood vessels namely arteries and veins
into the dialysate by osmotic process.
Dialysis Types
slide 5
Bacterial Growth in Dialysis Systems
Water treatment must eliminate Chemical Toxins Bacterial Contaminants Reverse Osmosis reduces bacteria and endotoxin levels But, bacteria escape to downstream sites and begin to proliferate If sanitation is inadequate, bacteria and endotoxin will reach
dangerous levels
slide 6
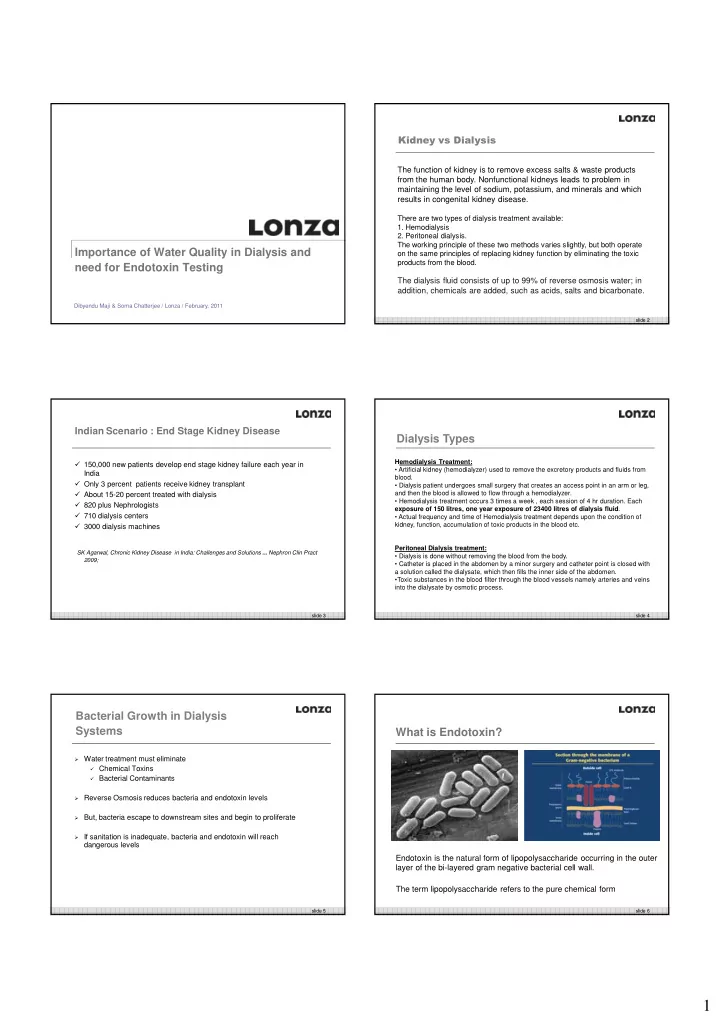
What is Endotoxin?
Endotoxin is the natural form of lipopolysaccharide occurring in the outer layer of the bi-layered gram negative bacterial cell wall. The term lipopolysaccharide refers to the pure chemical form