
1
Radiation Risks in low-Dose Imaging
Michael K O’Connor, Ph.D.
- Dept. of Radiology, Mayo Clinic
Radiation Units
Grey (Gy) = amount of radiation absorbed in any material Sievert (Sv) = estimates biological effect from the absorbed radiation Various weighting factors used to convert absorbed dose (in Grey) and dose to one organ (in Sievert) to “effective dose” to the whole body (in Sievert) e.g. Mammogram delivers absorbed dose of ~4 mGy to breast tissue. This gives an effective dose to the whole body
- f ~0.5 mSv
Converting radiation dose (mGy) to an estimate of its biological effect (mSv)
Head CT = 30 mGy to brain Digital mammogram = 4 mGy to breast tissue
+
Digital mammogram = 0.5 mSv Head CT = 2 mSv
Estimated biological effect of a head CT is 4 times that of a digital mammogram
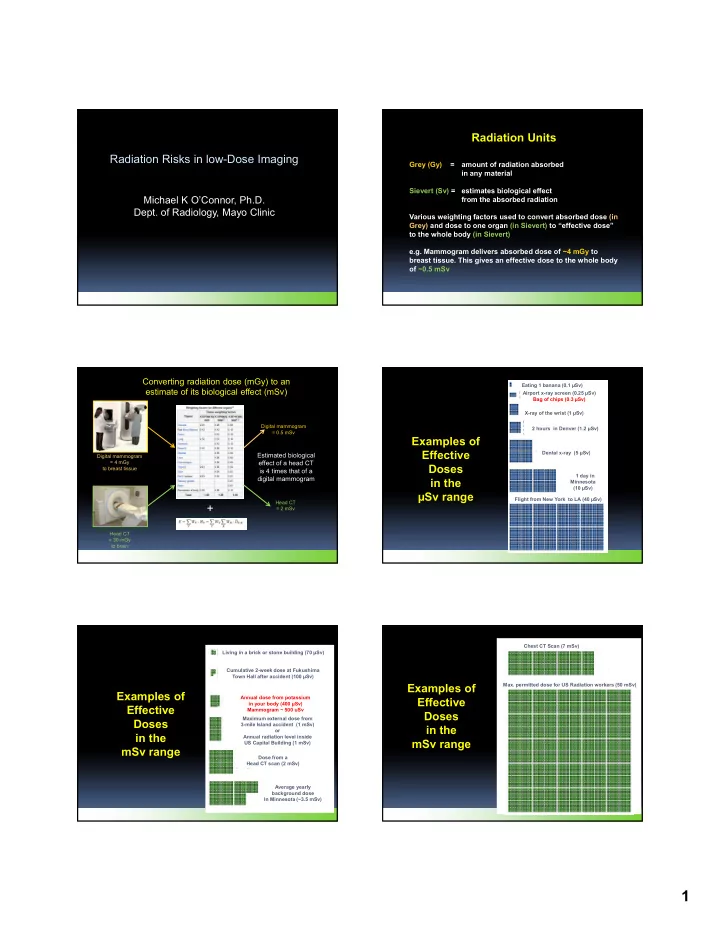
Examples of Effective Doses in the µSv range
Eating 1 banana (0.1 µSv) Dental x-ray (5 µSv) 2 hours in Denver (1.2 µSv) X-ray of the wrist (1 µSv) 1 day in Minnesota (10 µSv) Airport x-ray screen (0.25 µSv) Bag of chips (0.3 µSv) Flight from New York to LA (40 µSv)
Examples of Effective Doses in the mSv range
Living in a brick or stone building (70 µSv) Cumulative 2-week dose at Fukushima Town Hall after accident (100 µSv) Annual dose from potassium in your body (400 µSv) Mammogram ~ 500 uSv Maximum external dose from 3-mile Island accident (1 mSv)
- r
Annual radiation level inside US Capital Building (1 mSv) Dose from a Head CT scan (2 mSv) Average yearly background dose In Minnesota (~3.5 mSv)
Examples of Effective Doses in the mSv range
Chest CT Scan (7 mSv)
- Max. permitted dose for US Radiation workers (50 mSv)