SLIDE 29 Study nam e Outcom e Statistics for each study R ate ratio and 95% C I R ate Lower U pper ratio lim it lim it Z-Value p-Value B ea ucla ir et al. 2 00 5 # H
a tio n .10 3 .04 4 .23 9
.2 98 .00 A ra to & E rdo s 19 79 # H
a tio n .10 6 .06 2 .18 2
.1 40 .00 W a ldm a n & N e u m a n 19 8 4 # H
a tio n .20 1 .13 7 .29 6
.1 43 .00 D en ha m & A da m so n 19 7 1 # H
a tio n .26 2 .19 2 .35 7
.4 37 .00 M
97 4 # H
a tio n .28 3 .16 5 .48 5
.5 90 .00 M alm 19 71 # H
a tio n .29 4 .17 9 .48 4
.8 11 .00 D evito e t al. 1 97 8 # H
a tio n .35 5 .23 9 .52 8
.1 13 .00 P
n
ita & Jam e s 19 76 # H
a tio n .41 4 .26 9 .63 9
.9 90 .00 1 C ha ng e t al. 2 01 2 # H
a tio n .43 .31 8 .58
.5 19 .00 C arsw ell e t a
1 # H
a tio n .44 1 .38 1 .51 1 -1 0.98 3 .00 L ind ho lm 1 9 75 # H
a tio n .44 7 .29 9 .67
.8 99 .00 1 P en g et al. 2 01 1 # H
a tio n .46 9 .33 1 .66 6
.2 32 .00 R en e t a
1 1 # H
a tio n .74 2 .68 2 .80 8
.8 98 .00 T an e t a
81 # H
a tio n .80 .64 1 .99 9
.9 68 .04 9 1 B
rin e t a
9 8 # H
a tio n 1 .34 6 1 .13 7 1 .59 5 3 .44 1 .00 6 .38 1 .28 3 .51 3
.3 72 .00 0.1 0.2 0.5 1 2 5 10 Favours LA I Favours OA P
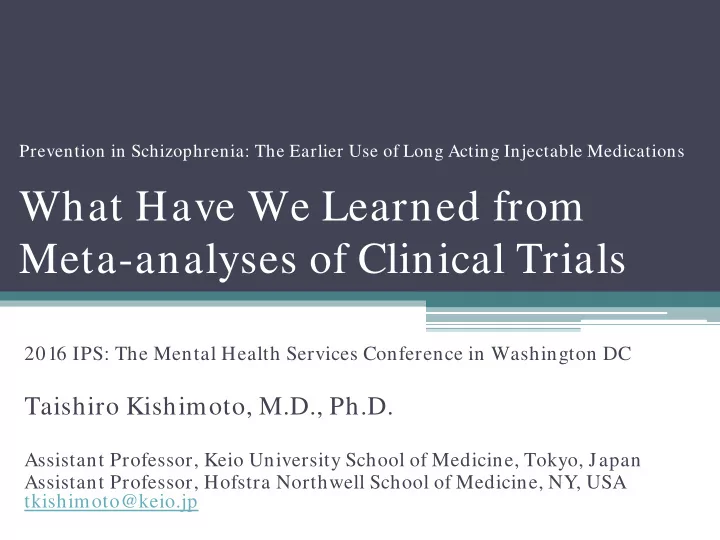
LAI vs. Oral Antipsychotics Mirror-Im age Studies [# of Hospitalization]
15 studies, 6396 person years Rate Ratio=0.38, 95%CI:0.28-0.51, p<0.0001 NNT=2
Kishimoto T et al. J Clin Psych 2013