
SLIDE 1
2/19/2014 1
1Basic Stroke Care
Airway Management Elevate Head of Bed 30 Degrees NPO Bedrails Up Fever Control Blood Sugar Control ASA 160-325mg PO (if no blood on CT) Reverse Anticoagulants DVT Prophylaxis (ward)
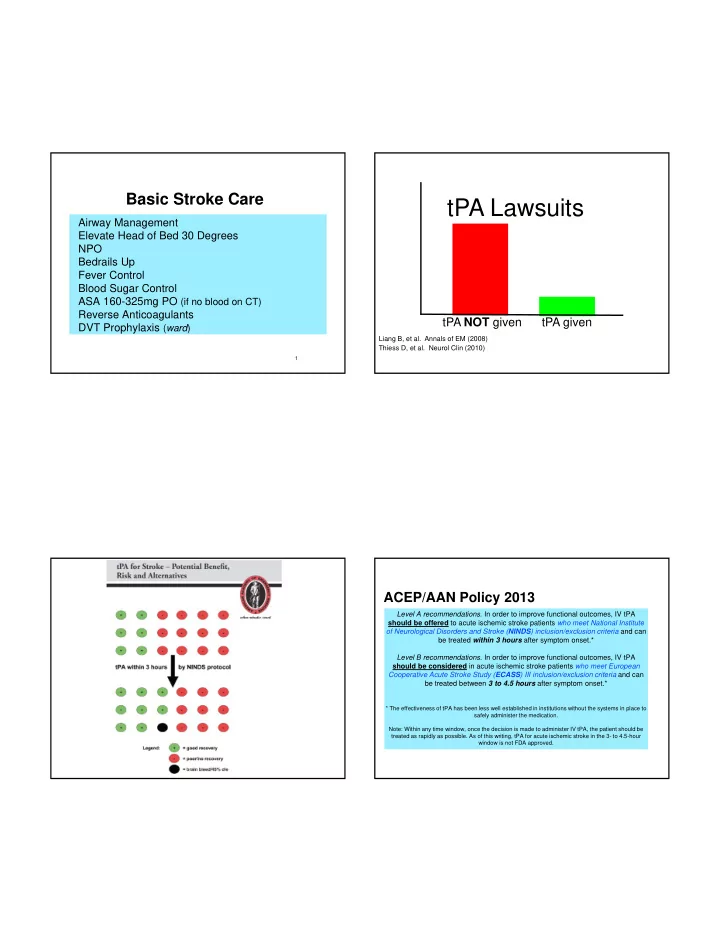
tPA NOT given tPA given
Liang B, et al. Annals of EM (2008) Thiess D, et al. Neurol Clin (2010)tPA Lawsuits
ACEP/AAN Policy 2013
Level A recommendations. In order to improve functional outcomes, IV tPA should be offered to acute ischemic stroke patients who meet National Institute- f Neurological Disorders and Stroke (NINDS) inclusion/exclusion criteria and can