
SLIDE 1
9/29/2016 1
TOBACCO CESSATION: A REVIEW OF CURRENT PRACTICES AND AN UPDATE TO E‐CIGARETTES
Jessica Kerwin, PharmD PGY‐2 Ambulatory Care Resident UNM College of Pharmacy jlkerwin@salud.unm.edu
Objectives
- Discuss the “5 A’s” model for treating tobacco use and
dependence.
- Given a patient case, identify a patient’s readiness to
quit smoking or using tobacco products.
- Evaluate a patient case to determine the best smoking
cessation product based on patient‐specific factors.
- Describe recent updates to the regulation of
electronic cigarettes and how these could impact smoking cessation.
Tobacco Use1
- Leading cause of preventable
and premature death
- Kills an estimated 443,000
Americans each year
- Costs $96 billion in direct
medical costs annually
- Every day in the US, 3,800 Americans under the
age of 18 smoke their first cigarette
- Decreases in smoking rates have stalled
Tobacco Use1
- Prevalence of cigarette smoking is highest
among lower socioeconomic youth
- Smokeless tobacco use is increasing among
white high school males
- Rates lower in women but gap is decreasing
- Concurrent use of multiple tobacco products is
common, with 50% of White and Hispanic males reporting using more than one product
- Nearly 7 out of every 10 adult cigarette users
reports that they want to quit smoking entirely
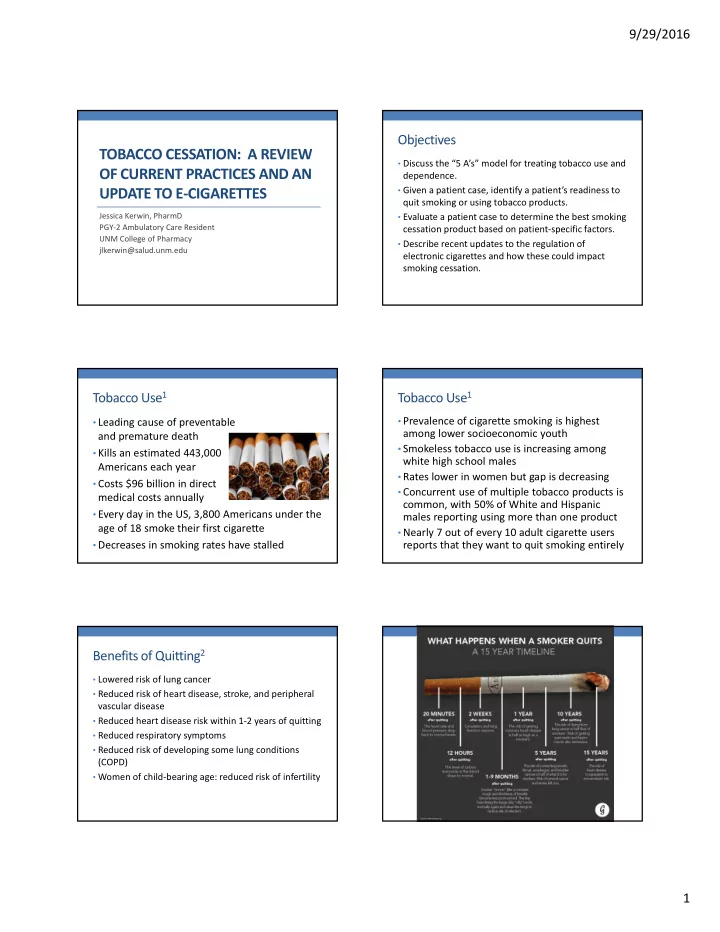
Benefits of Quitting2
- Lowered risk of lung cancer
- Reduced risk of heart disease, stroke, and peripheral
vascular disease
- Reduced heart disease risk within 1‐2 years of quitting
- Reduced respiratory symptoms
- Reduced risk of developing some lung conditions
(COPD)
- Women of child‐bearing age: reduced risk of infertility